This document discusses acute decompensated heart failure (ADHF), including:
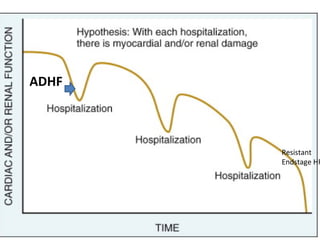
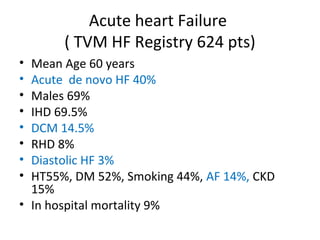
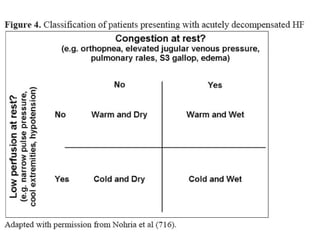
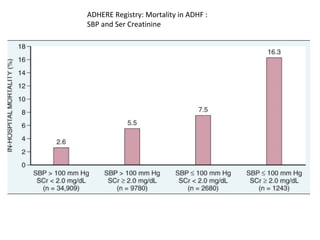
1. ADHF is characterized by rapidly developing symptoms of new or worsening chronic heart failure requiring hospitalization. It carries a high risk of rehospitalization and mortality.
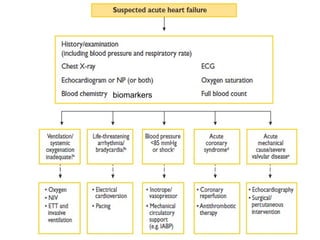
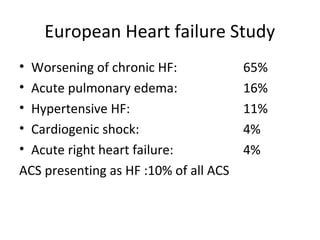
2. Causes of ADHF include non-adherence to medications, acute myocardial ischemia, arrhythmias, infections, and other cardiovascular disorders.
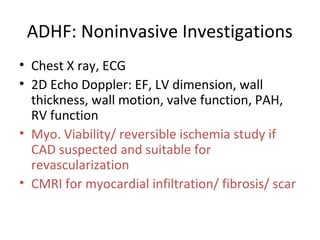
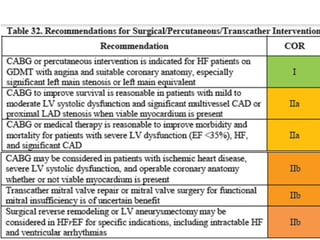
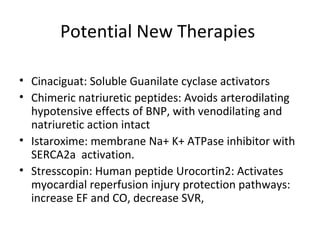
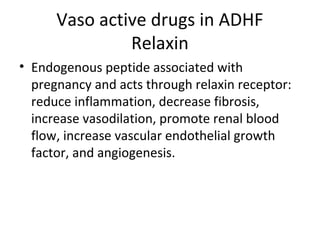
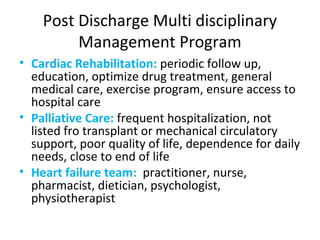
3. Management involves aggressive diuresis, treatment of underlying causes, optimization of disease-modifying medications, and consideration of inotropes or mechanical circulatory support for severe cases.
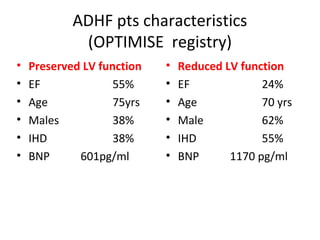
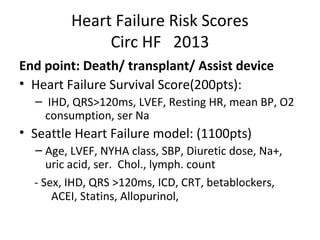
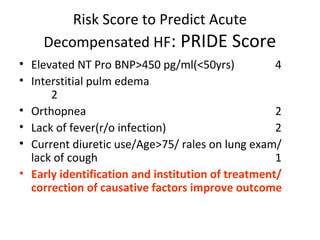
4. Biomarkers like BNP are useful for diagnosis, assessing severity, and guiding therapy, while















































![[20170216][Journal Club][Enhanced recovery pathways versus standard care afte...](https://cdn.slidesharecdn.com/ss_thumbnails/20170216journalclub-171114232901-thumbnail.jpg?width=640&height=640&fit=bounds)




























































