Download to read offline







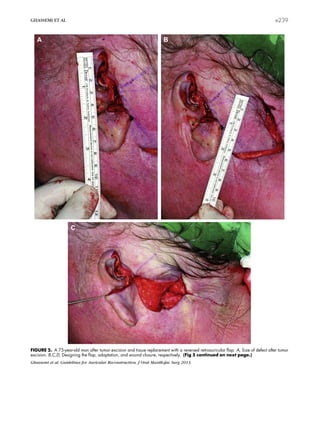

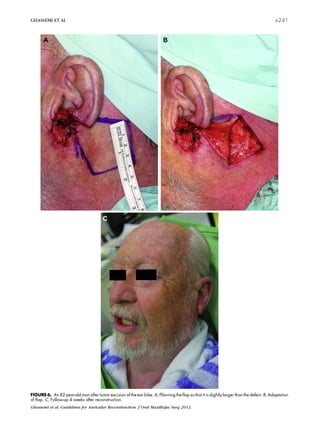


This document discusses surgical techniques for reconstructing auricular defects of different sizes. It summarizes the experience of surgeons in treating 75 patients over 10 years. For defects less than one-fourth the vertical ear size, primary closure is sufficient. For larger defects up to three-fourths the size, a reversed retroauricular flap is often used successfully. For defects exceeding three-fourths the size, an implant-retained prosthesis is preferred. The location, size, and tissue involved in the defect, as well as the patient's condition, determine the most appropriate reconstruction method.

















































































