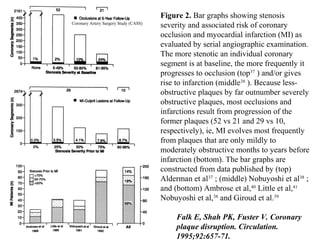
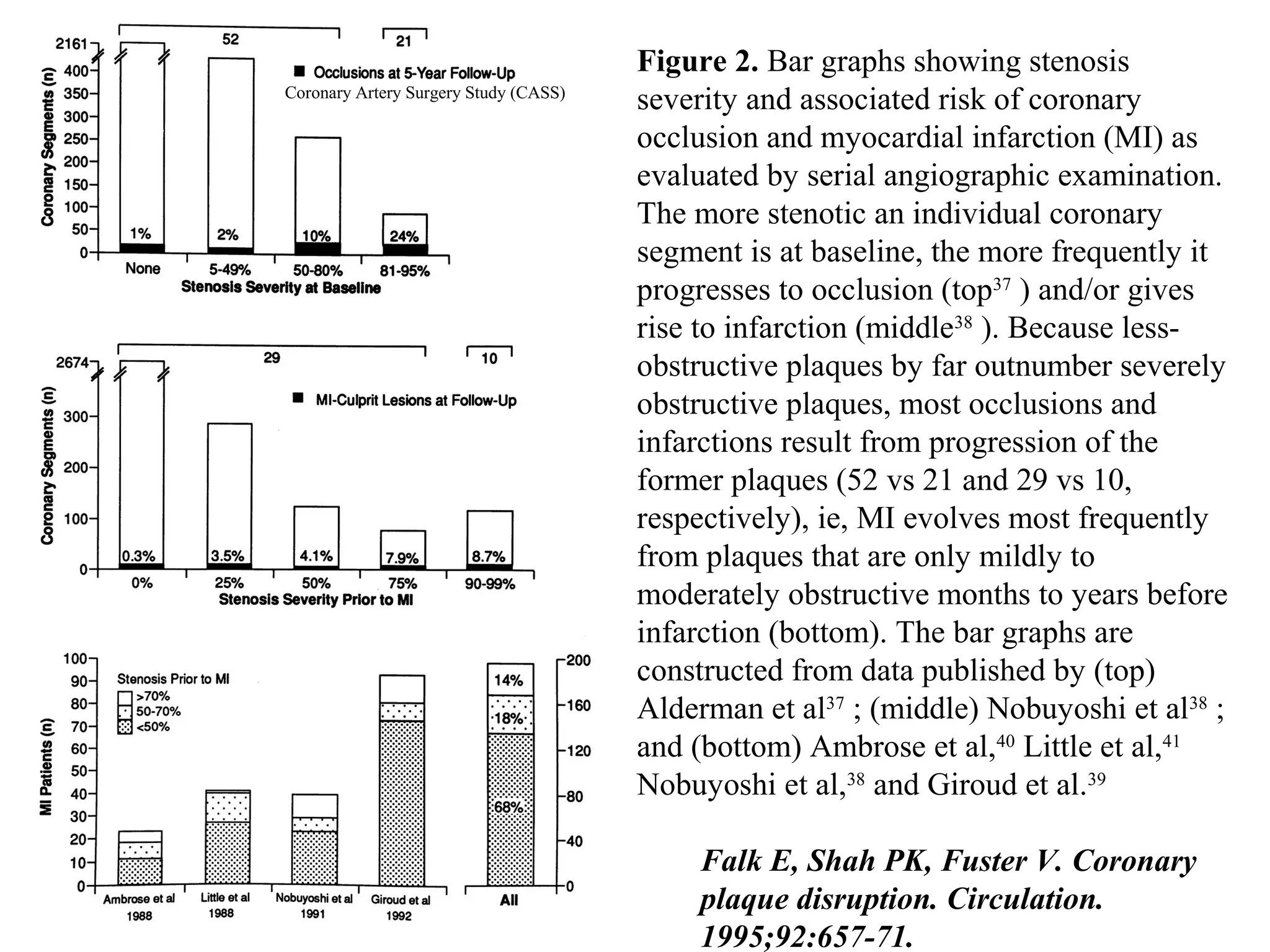
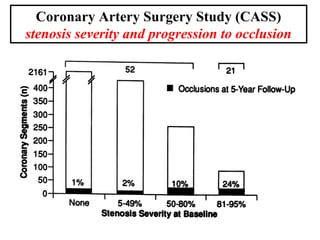
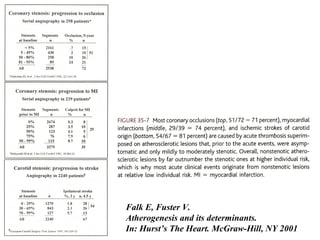
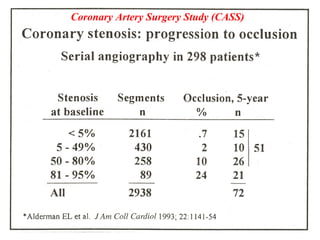
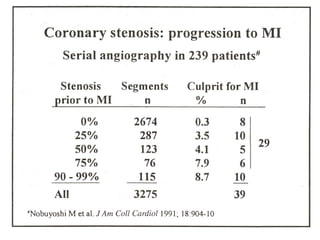
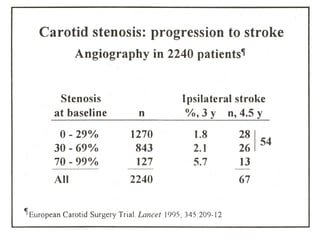
The more stenotic a coronary segment is at baseline, the more likely it is to progress to occlusion or myocardial infarction. Less obstructive plaques, which far outnumber severely obstructive plaques, are responsible for most occlusions and infarctions because they are more likely to progress. Myocardial infarction often results from plaques that were only mildly or moderately obstructive months or years prior.























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)















