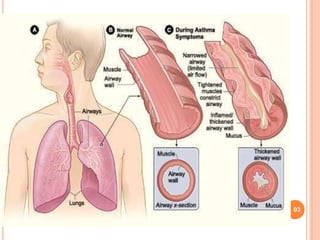


This document provides an overview of asthma, including: - Asthma is a chronic inflammatory disease of the airways characterized by airway inflammation and hyperresponsiveness leading to wheezing, coughing, chest tightness, and shortness of breath. - Risk factors include family history, allergy, airway irritants, stress, infections, cold air, air pollution, and certain drugs. - Symptoms include recurrent wheezing, chest tightness, breathlessness, and cough. Diagnosis involves patient history, physical exam, pulmonary function tests, and allergy tests. - Treatment focuses on relieving symptoms acutely with oxygen, bronchodilators, steroids, and preventing