The document summarizes a case study on a 2-year old female patient (H.A) admitted to the hospital for a brain tumor. Key details include:
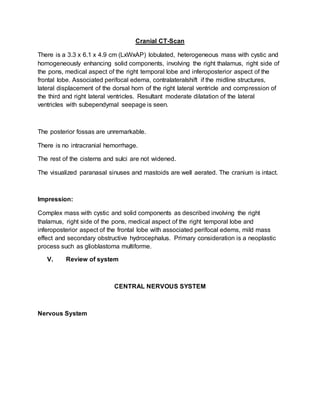
- H.A was admitted with complaints of headache, vomiting, fever and seizures. Previous tests showed a brain tumor.
- Her current vital signs show an elevated temperature of 40.0C, respiratory rate of 30 bpm, and heart rate of 160 bpm.
- The case study objectives are to understand H.A's condition, provide treatment, educate her family, and formulate a nursing care plan.