Download as PDF, PPTX


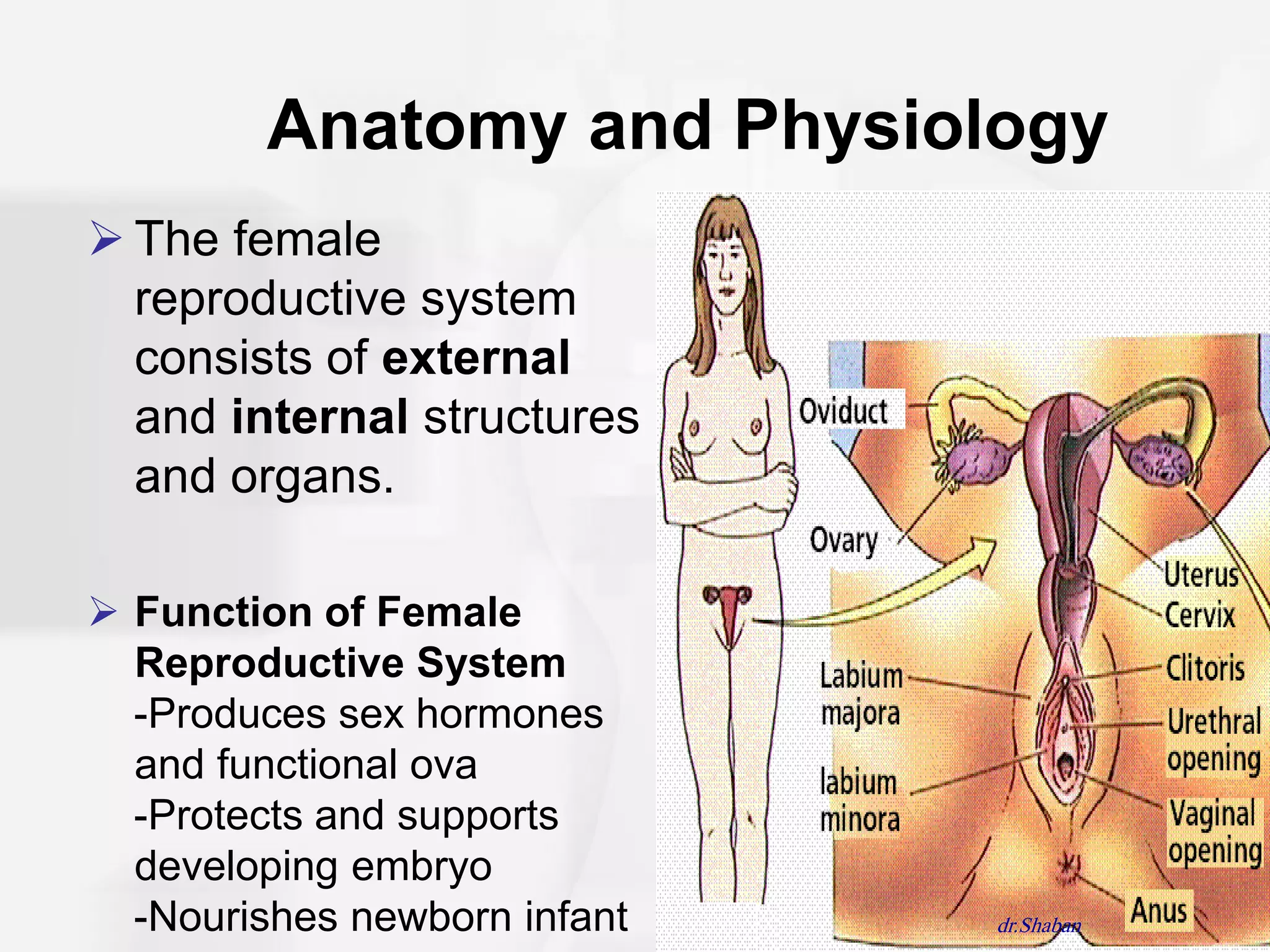
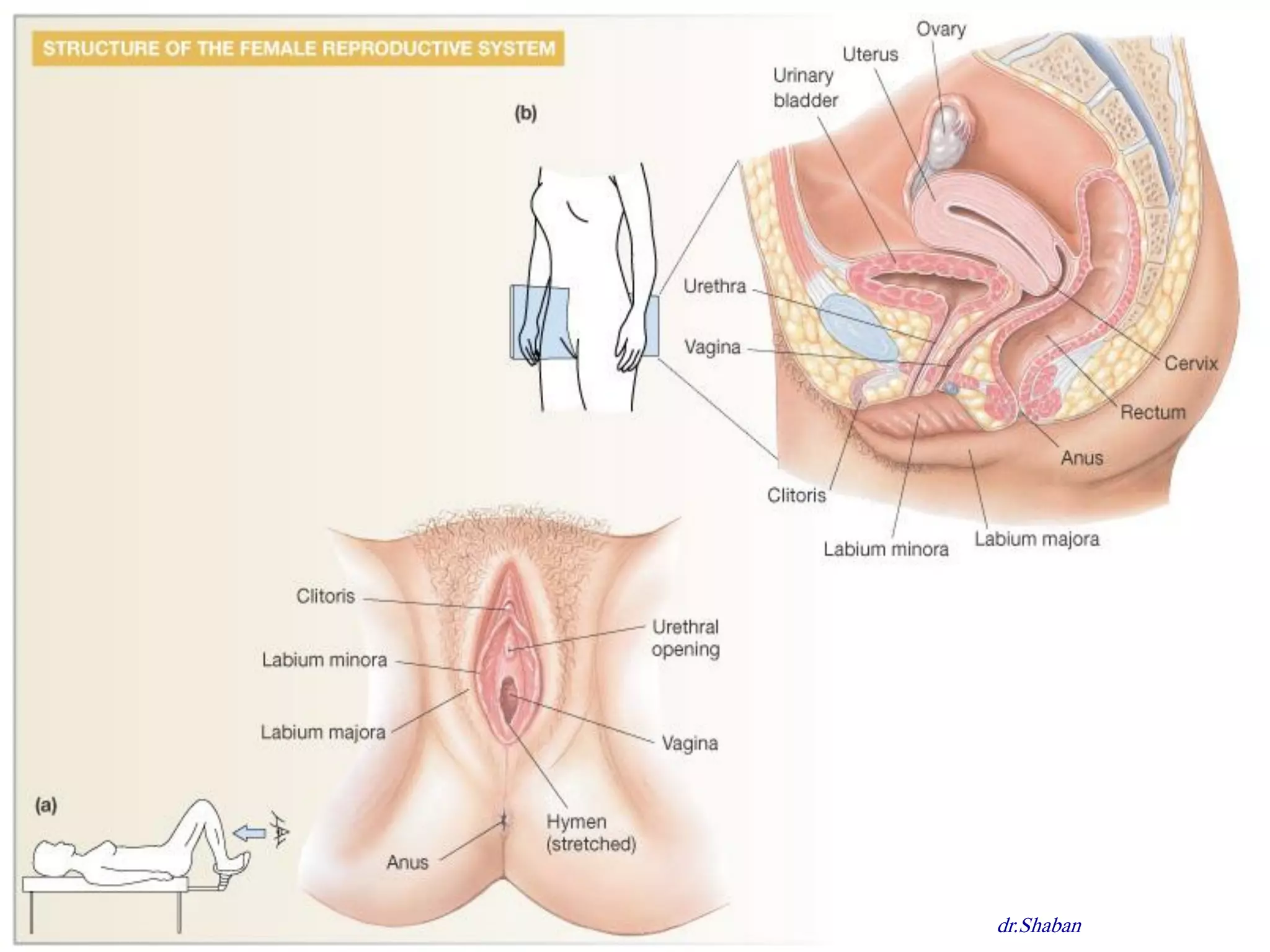
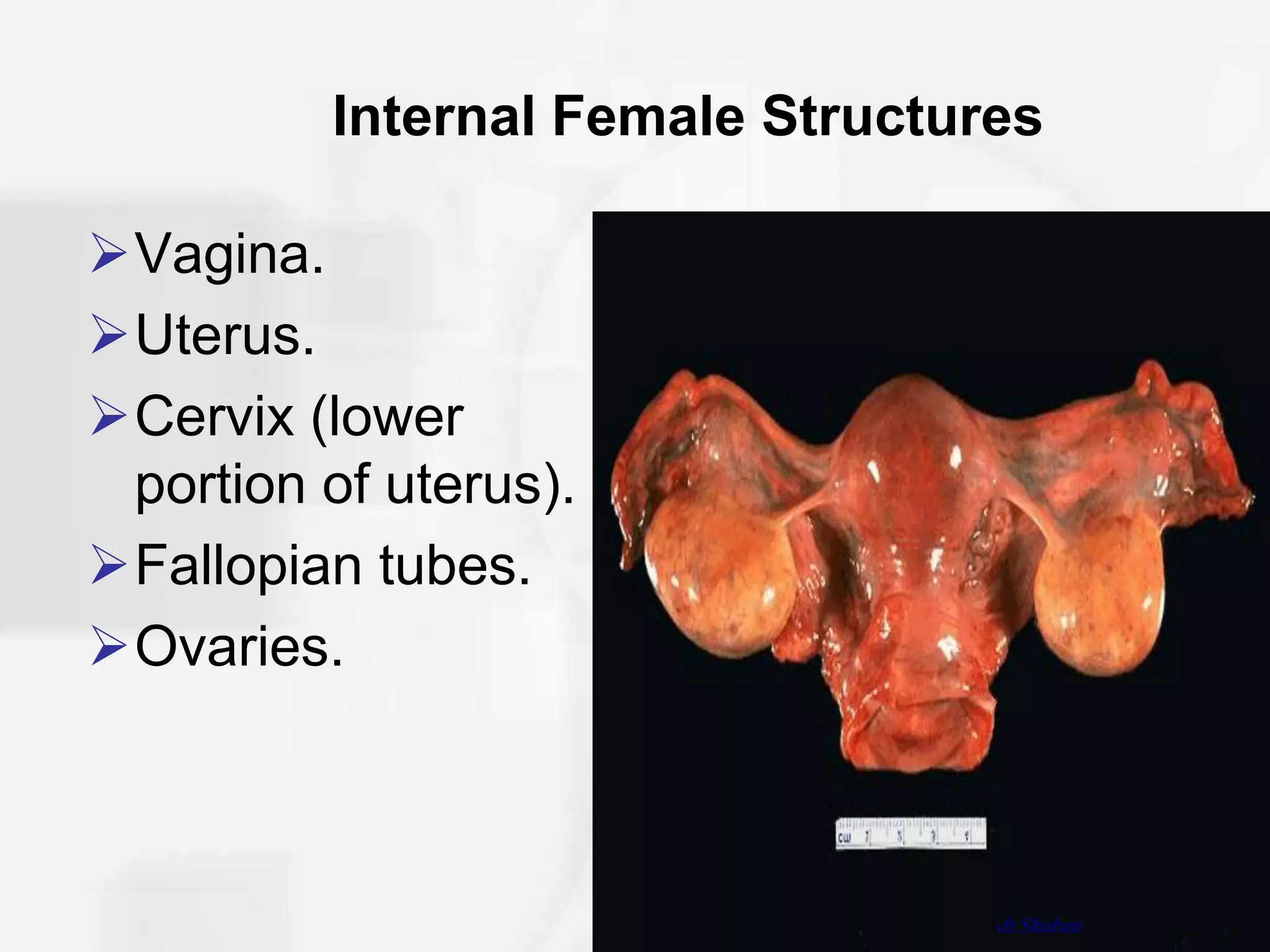
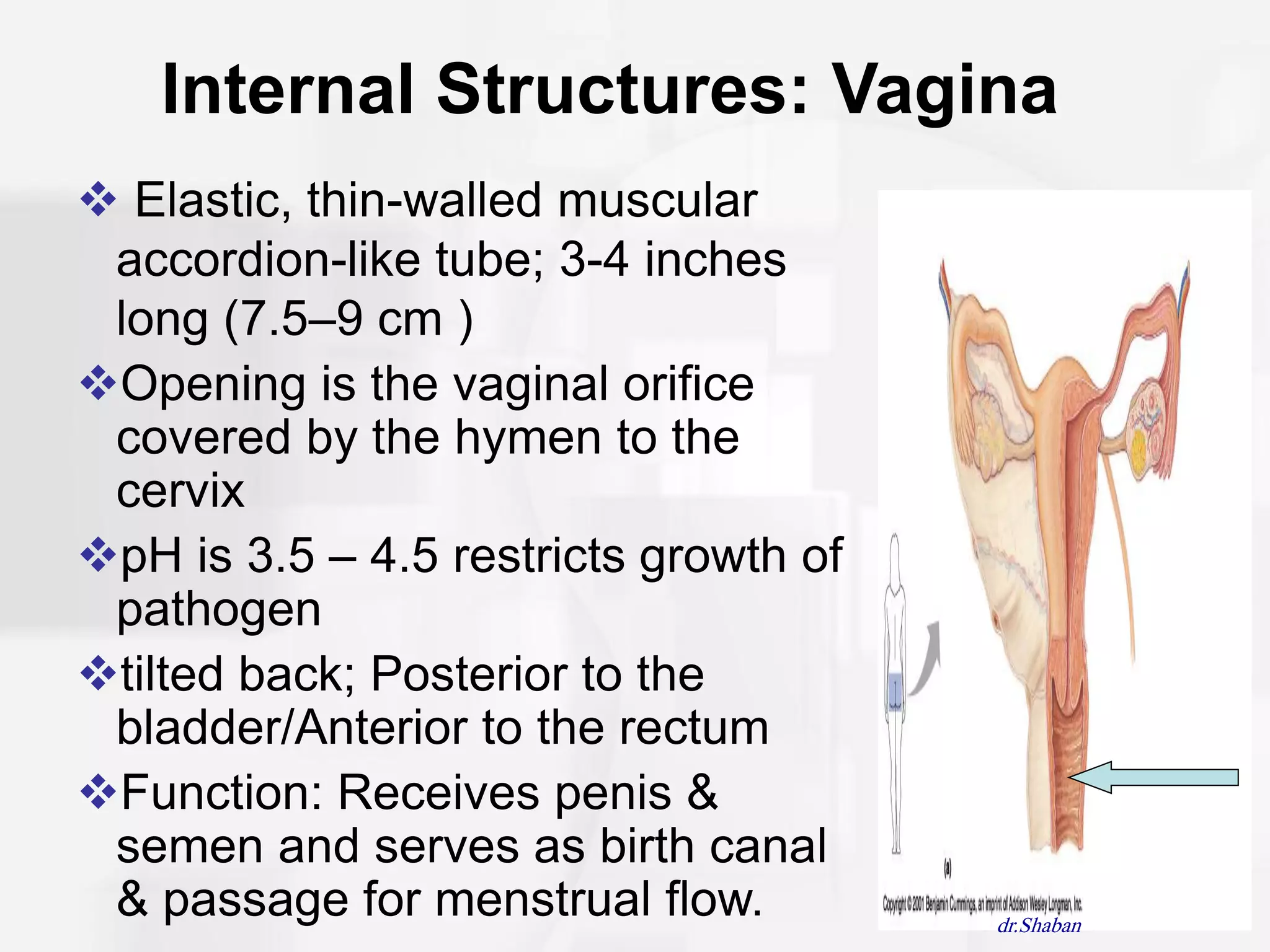
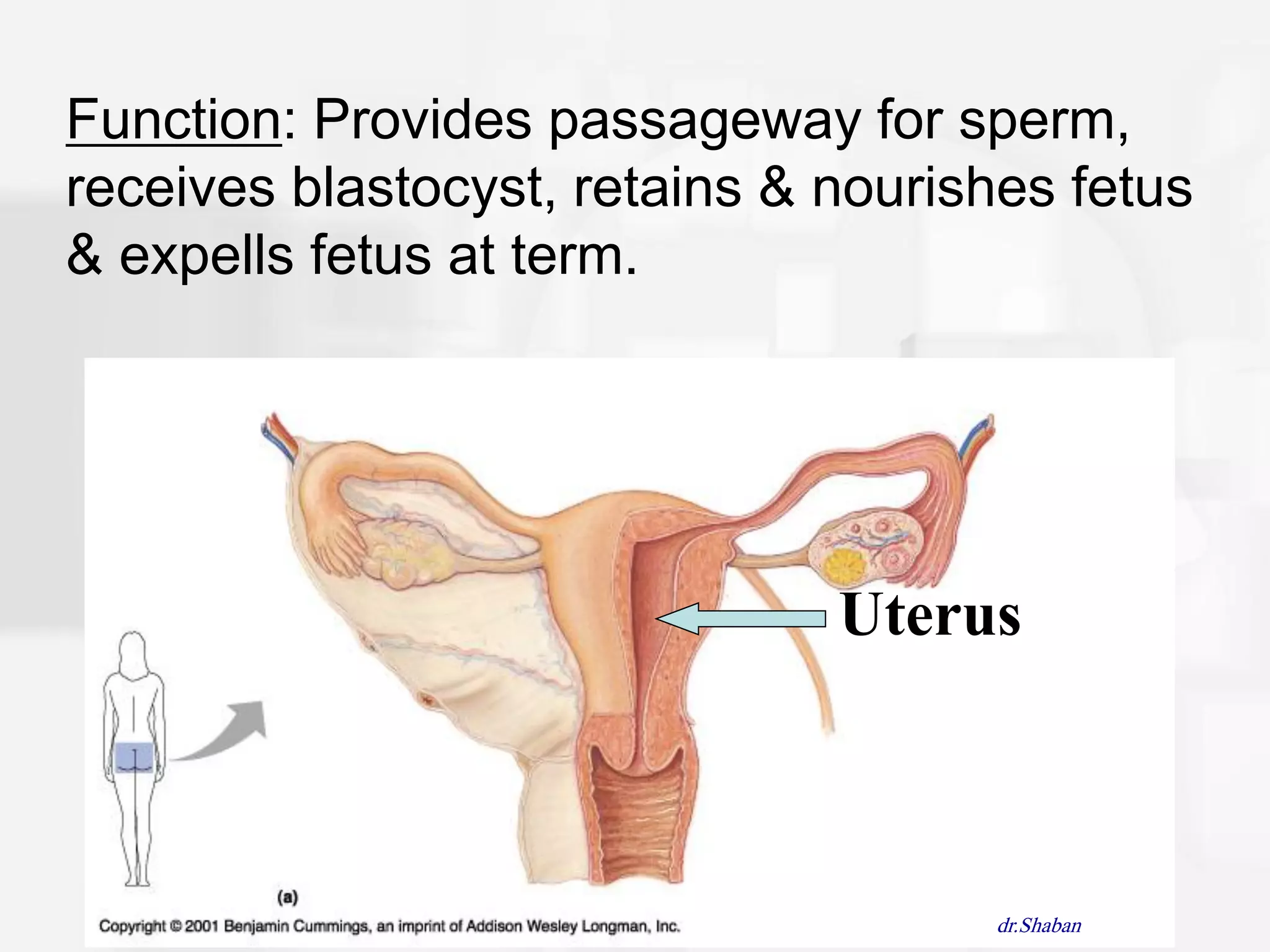
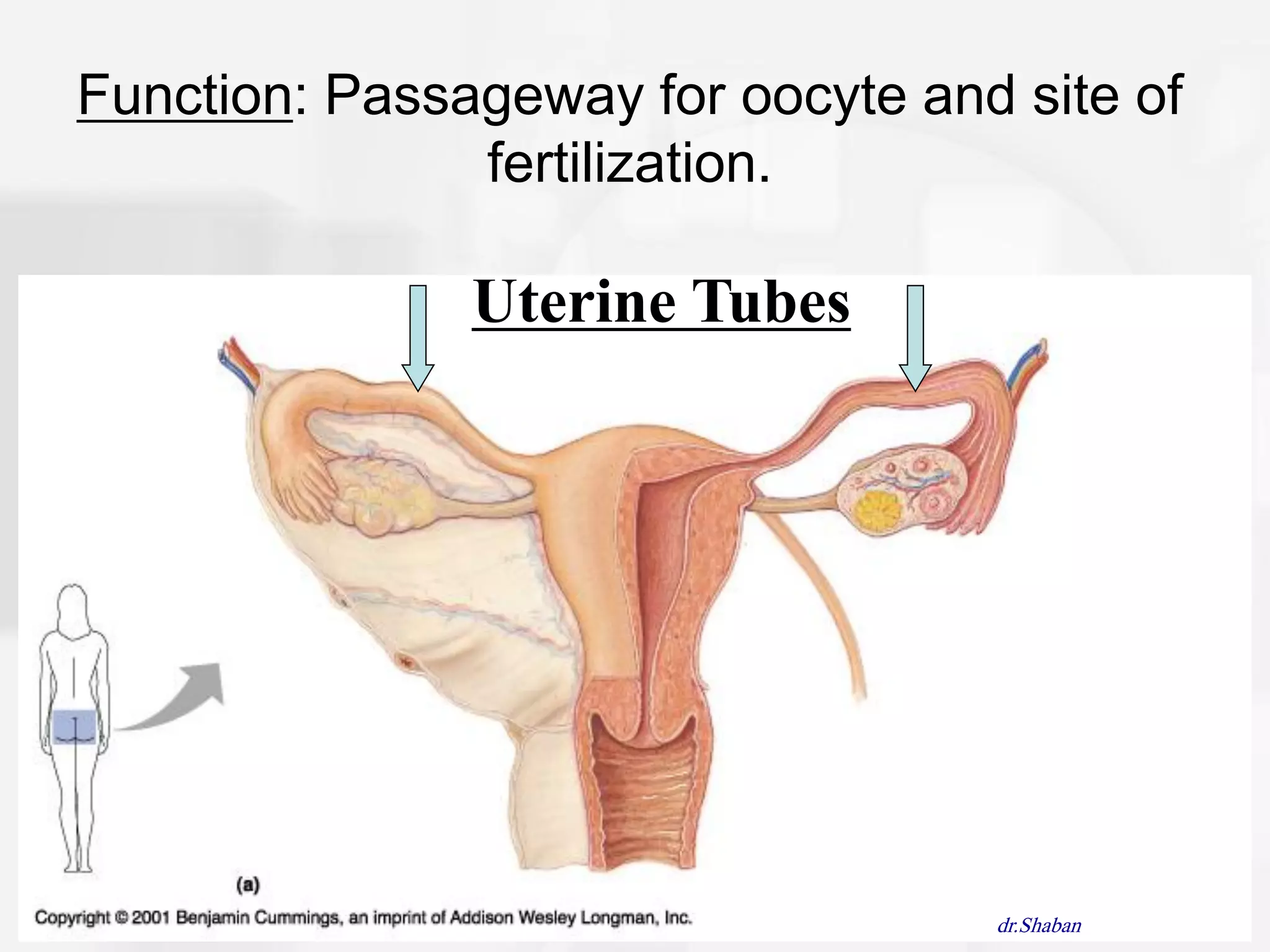
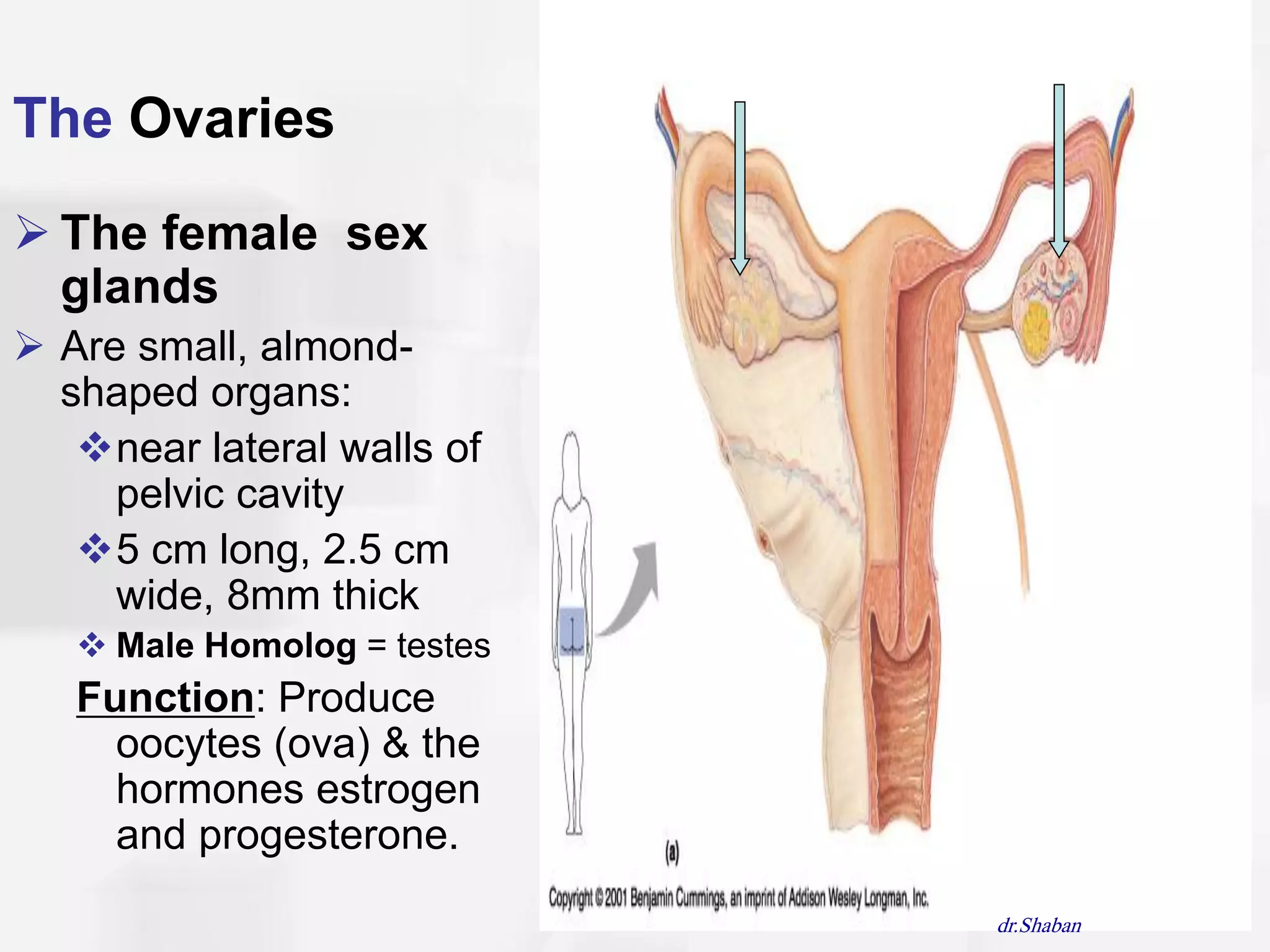
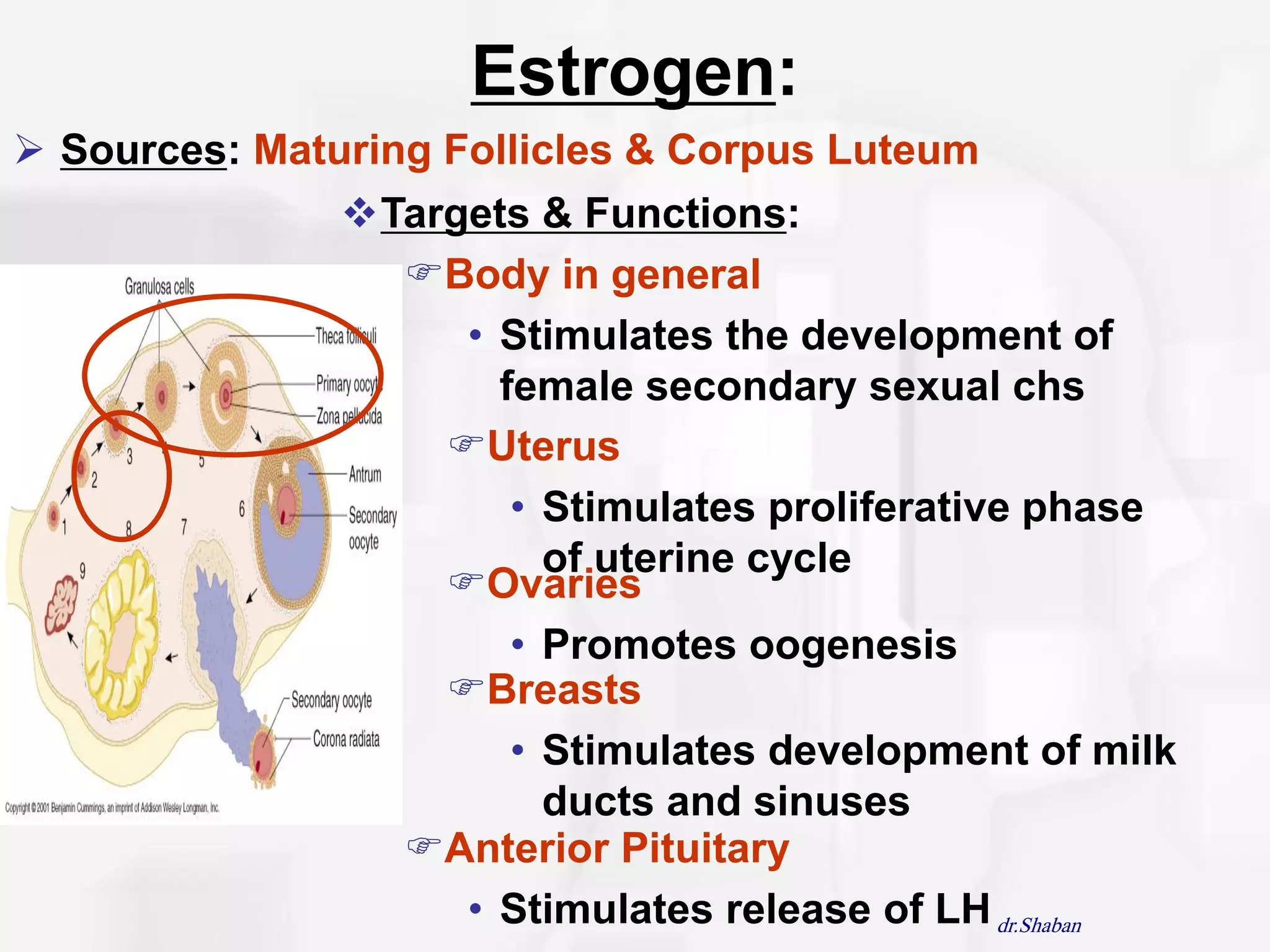
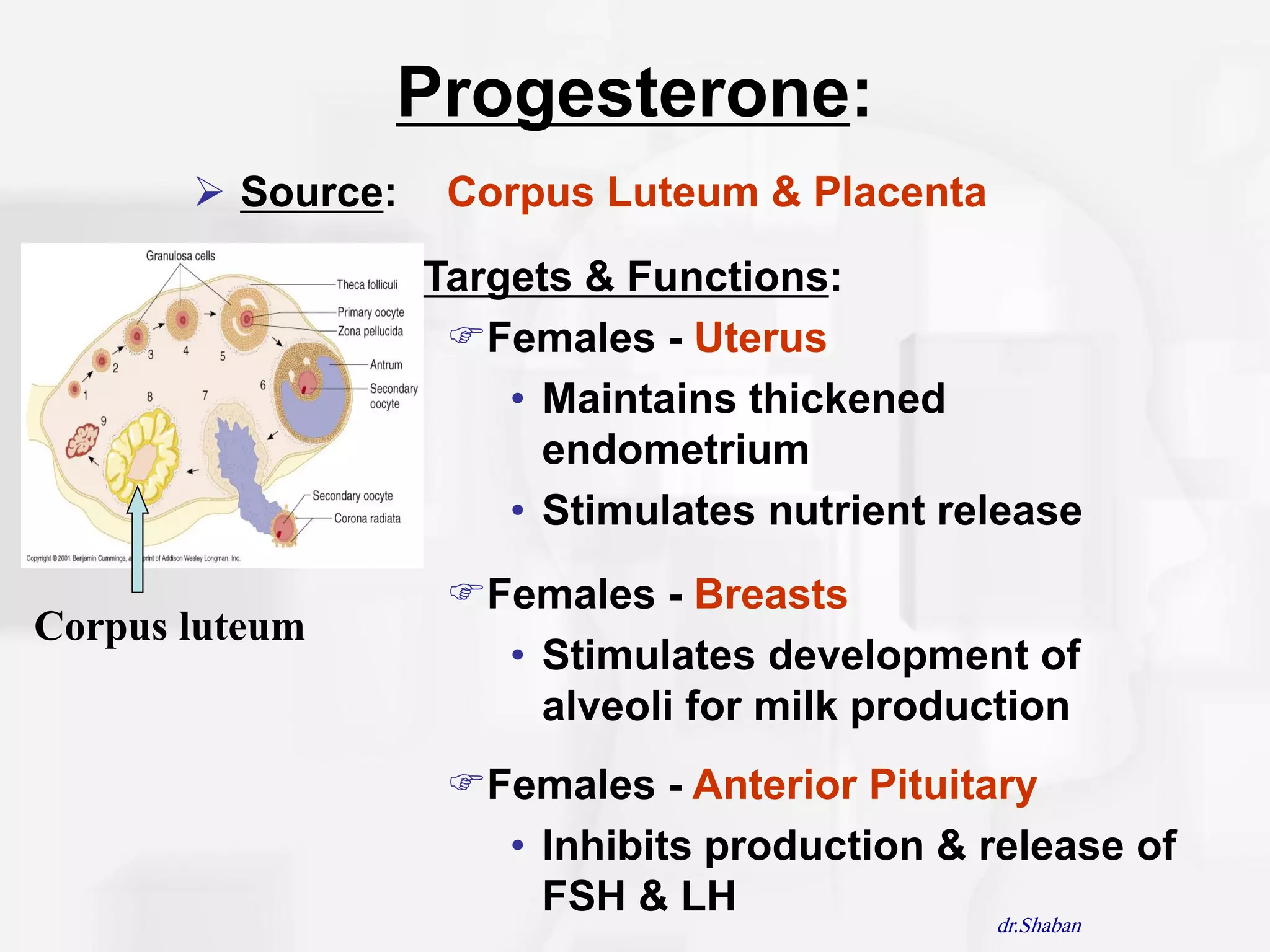
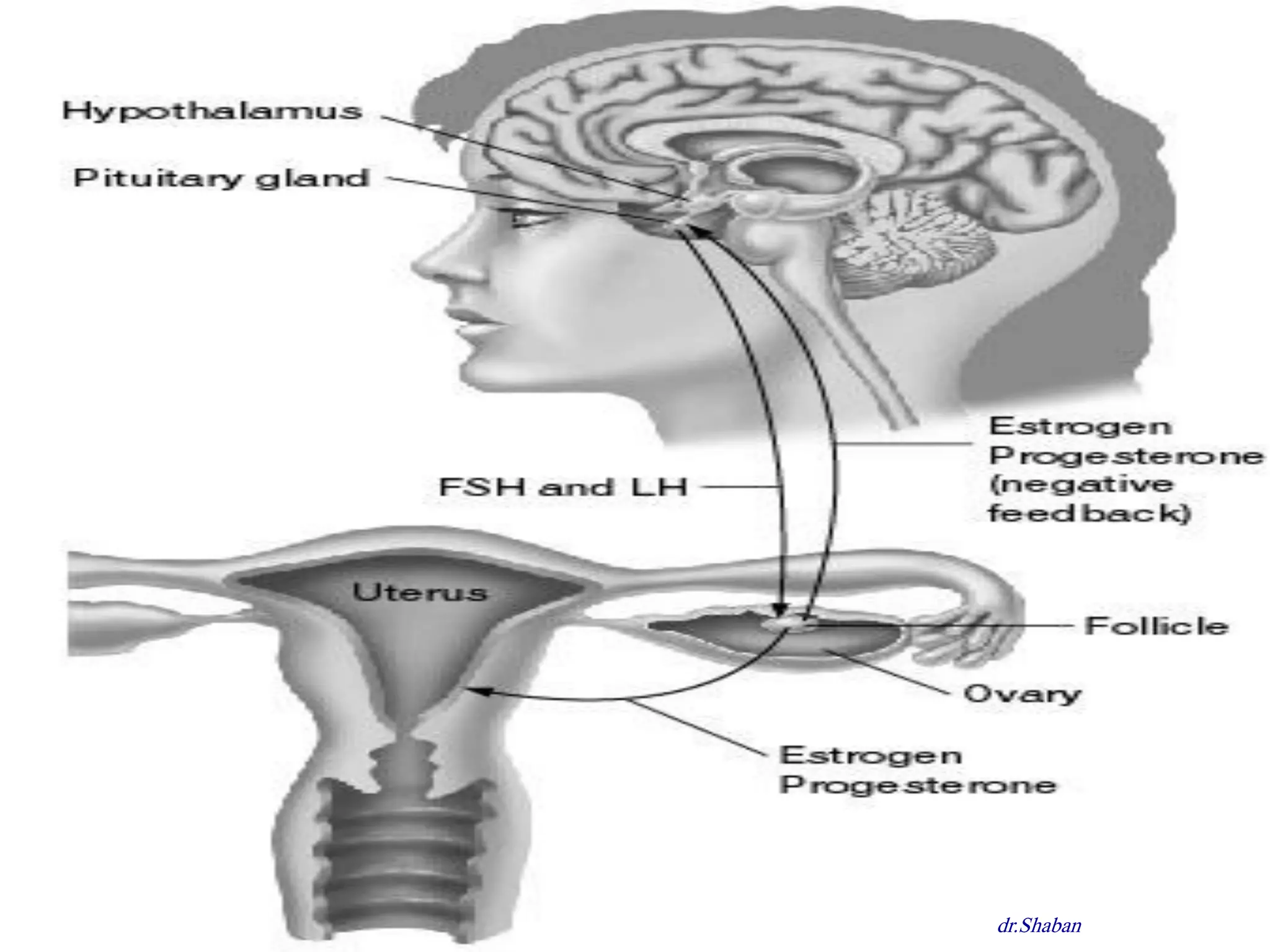
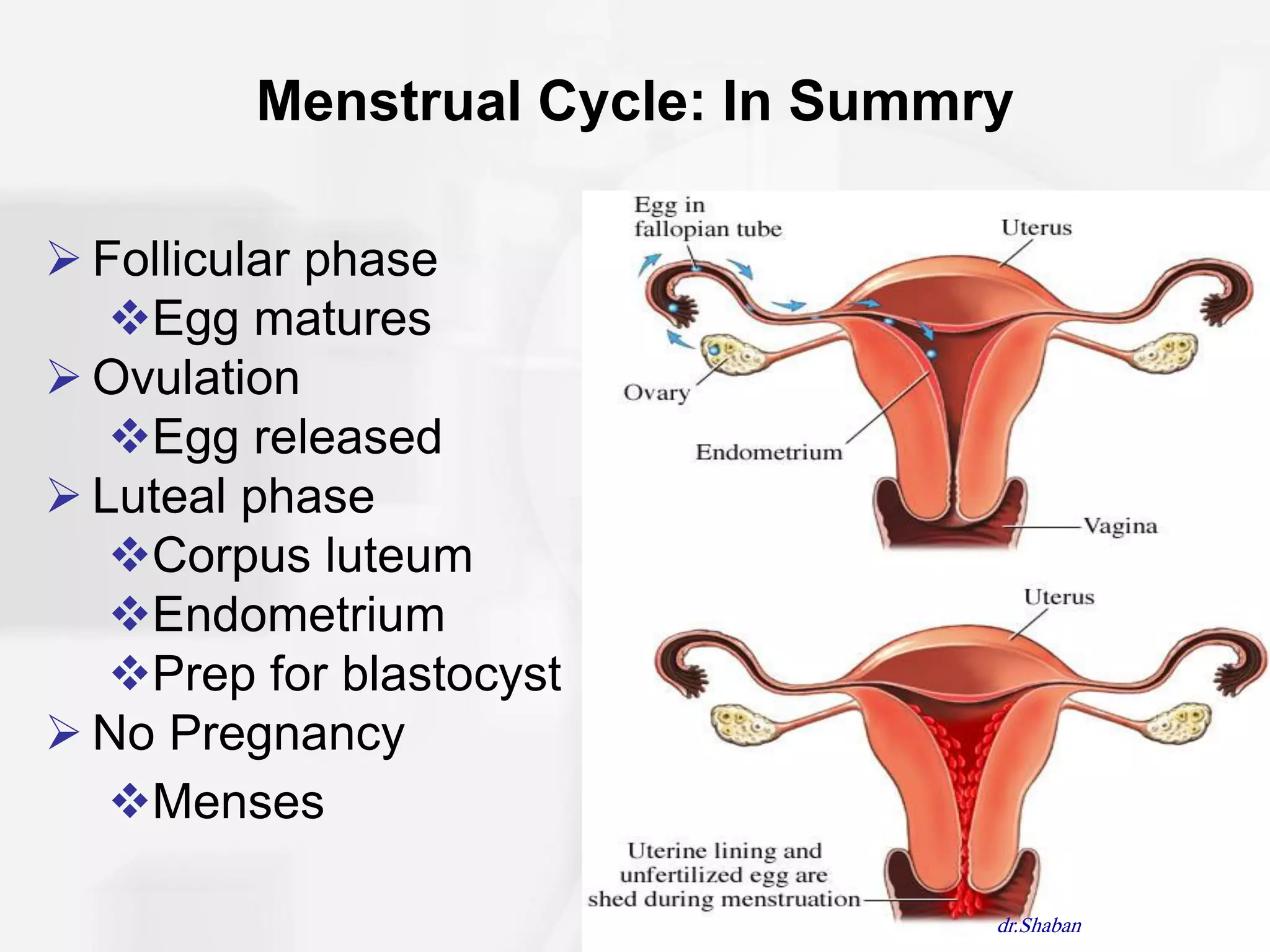
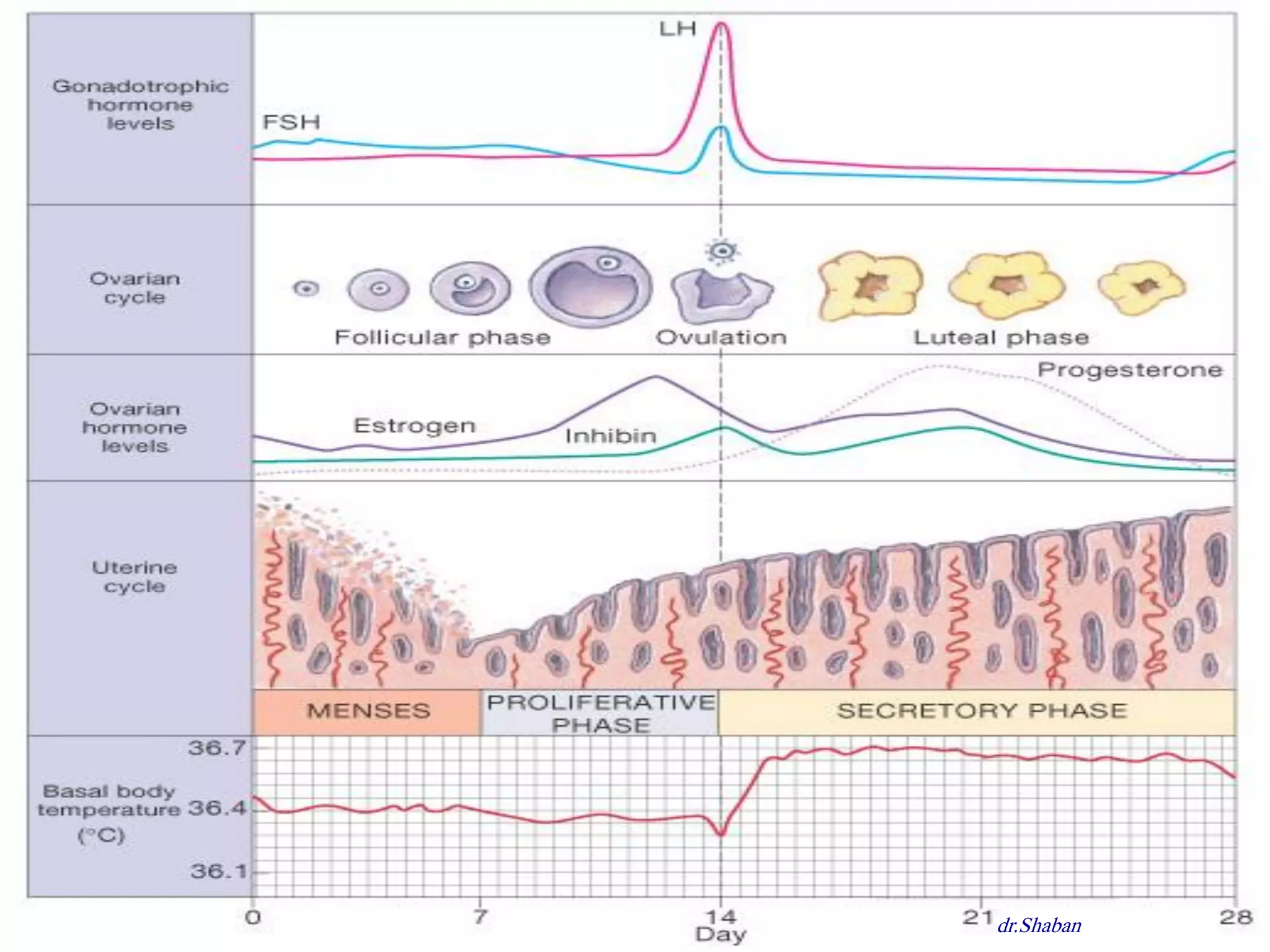

The document discusses the female reproductive system, including both external and internal structures. It describes the female organs such as the ovaries, uterus, vagina, and breasts. It explains the menstrual cycle in females, including the follicular, ovulation, and luteal phases. It also discusses common menstrual problems like premenstrual syndrome, amenorrhea, dysmenorrhea, menorrhagia, and metrorrhagia.














































































