Download as PDF, PPTX




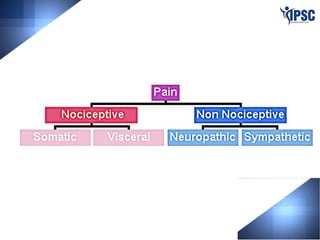
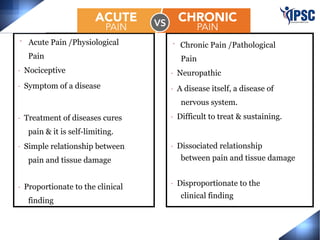
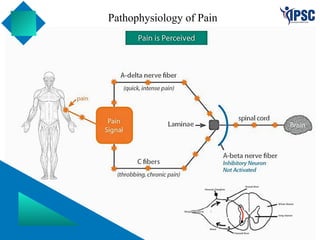
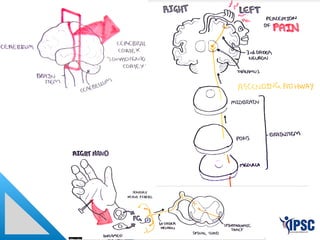
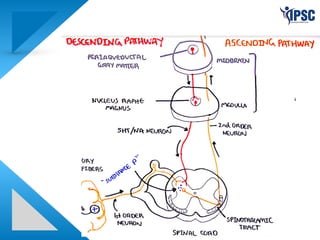
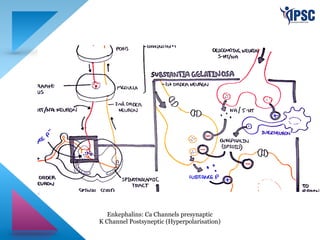
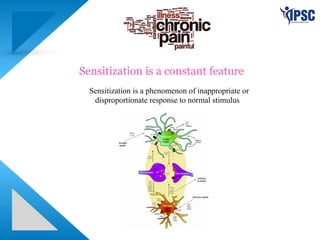




The document discusses pain management, emphasizing the distinction between acute and chronic pain, the pathophysiology of pain, and the role of interventional pain management techniques. It highlights the importance of understanding the psychological aspects of pain and the physiological mechanisms such as sensitization. Additionally, it notes that interventional pain management is a recognized medical specialty aimed at providing effective treatment options for various pain conditions.























































































