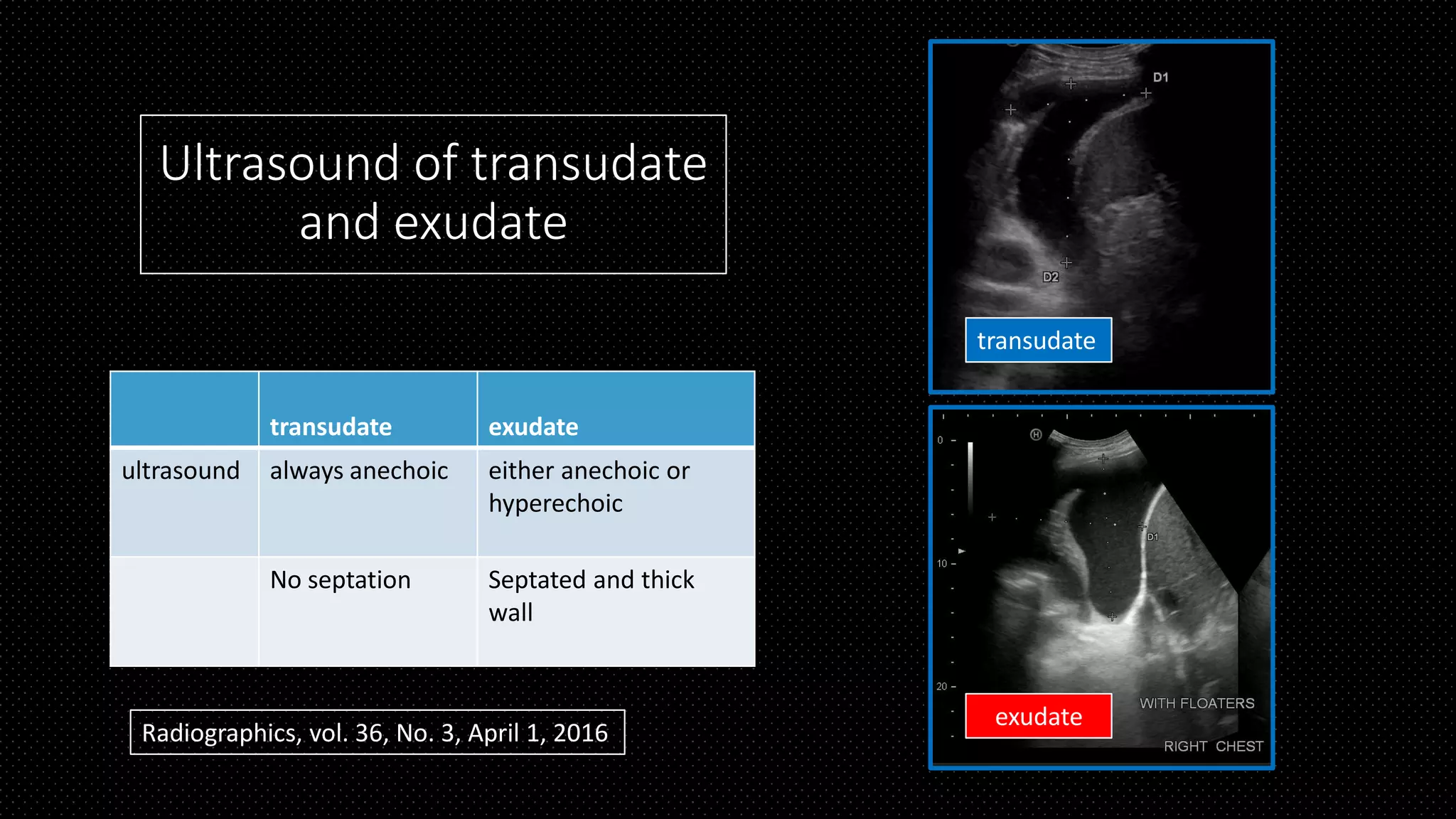
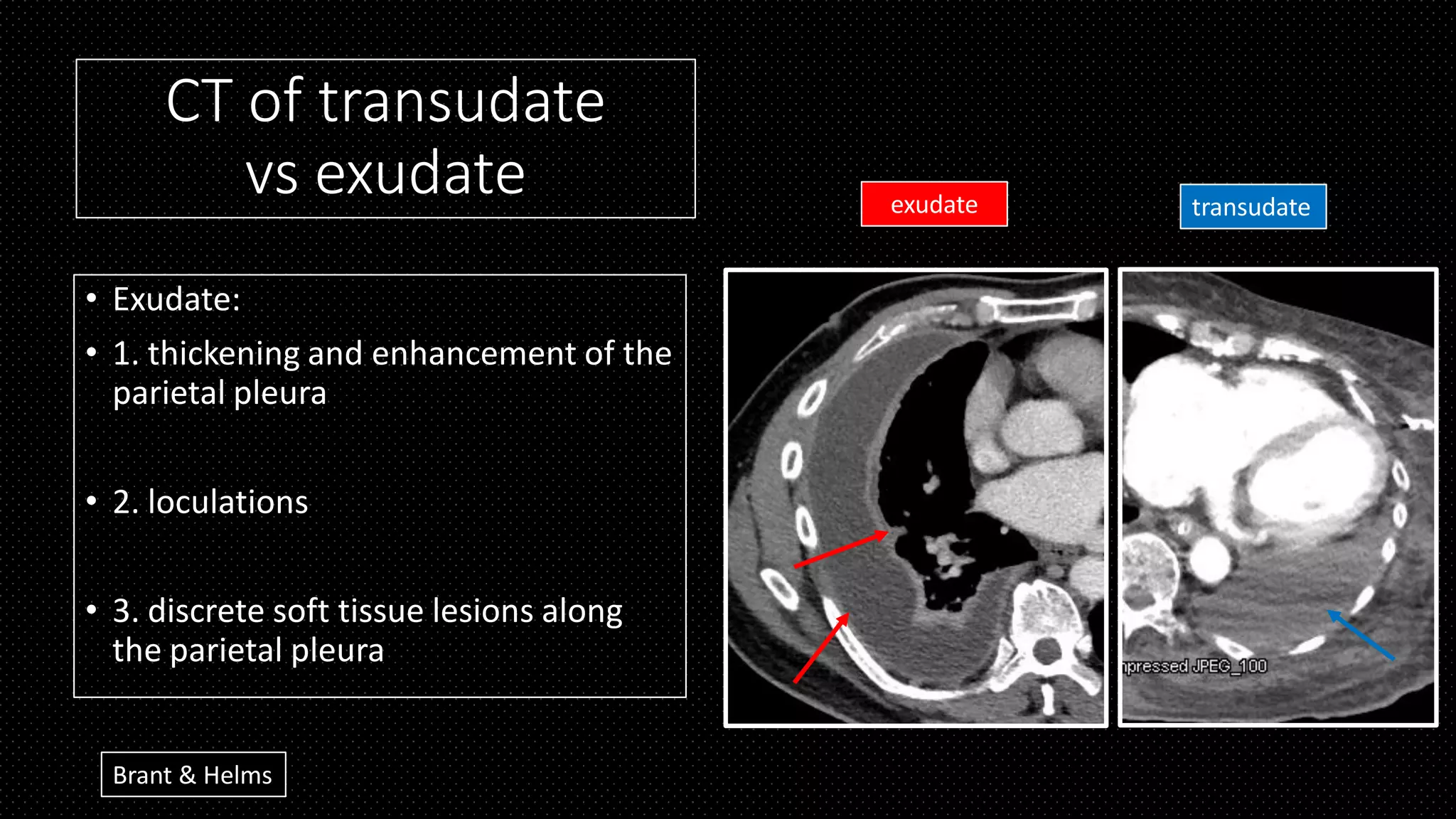
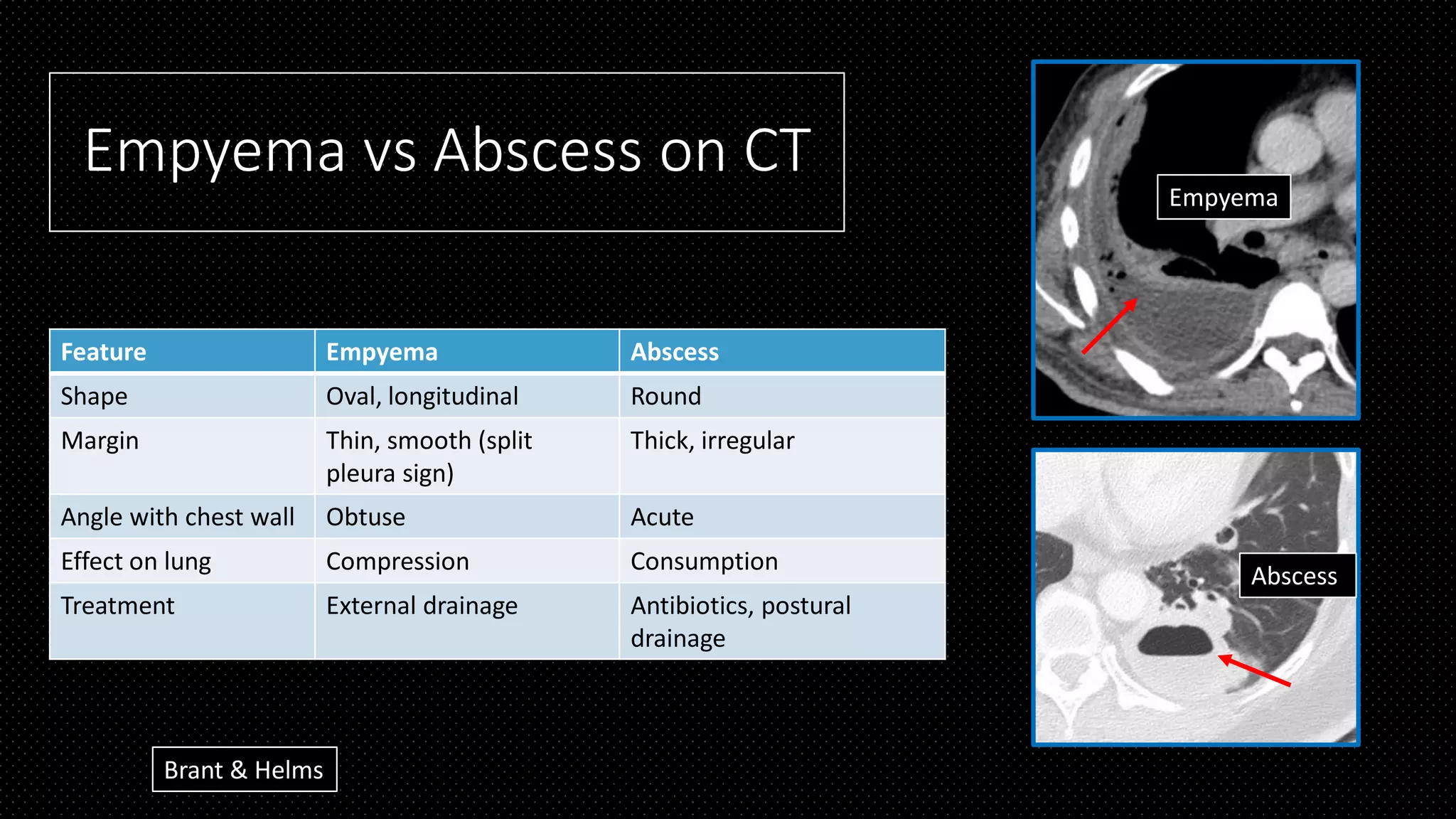
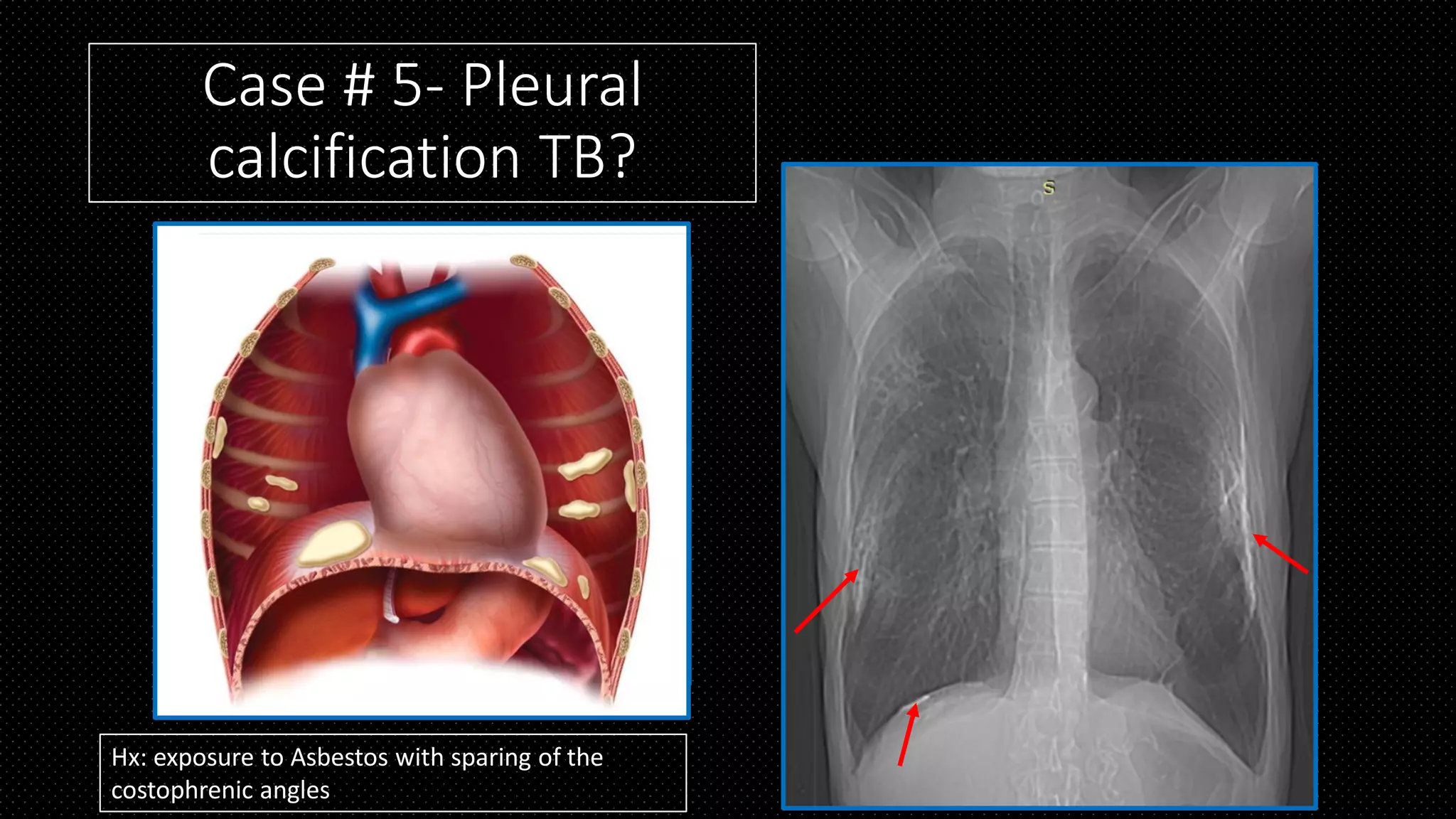
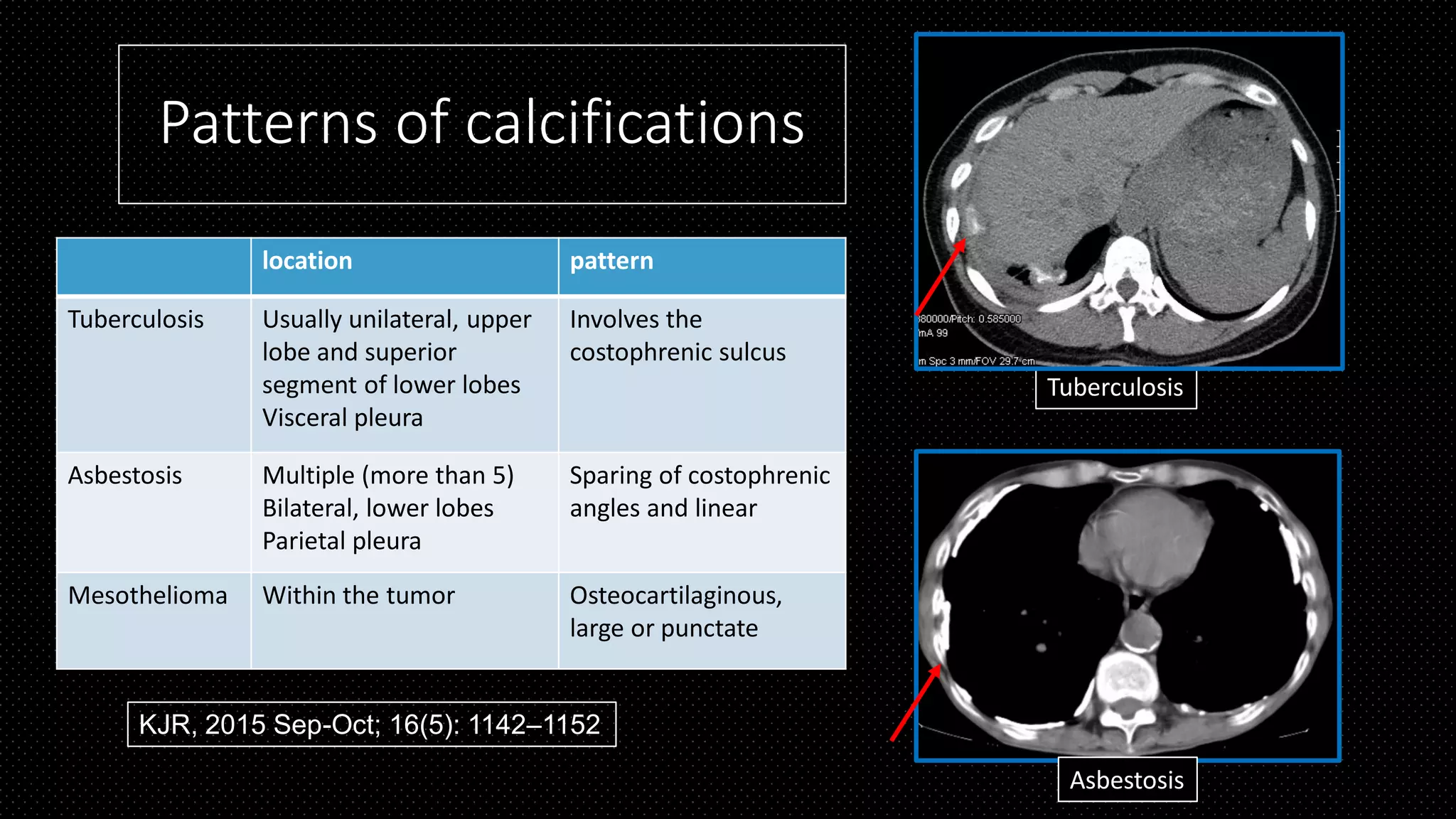
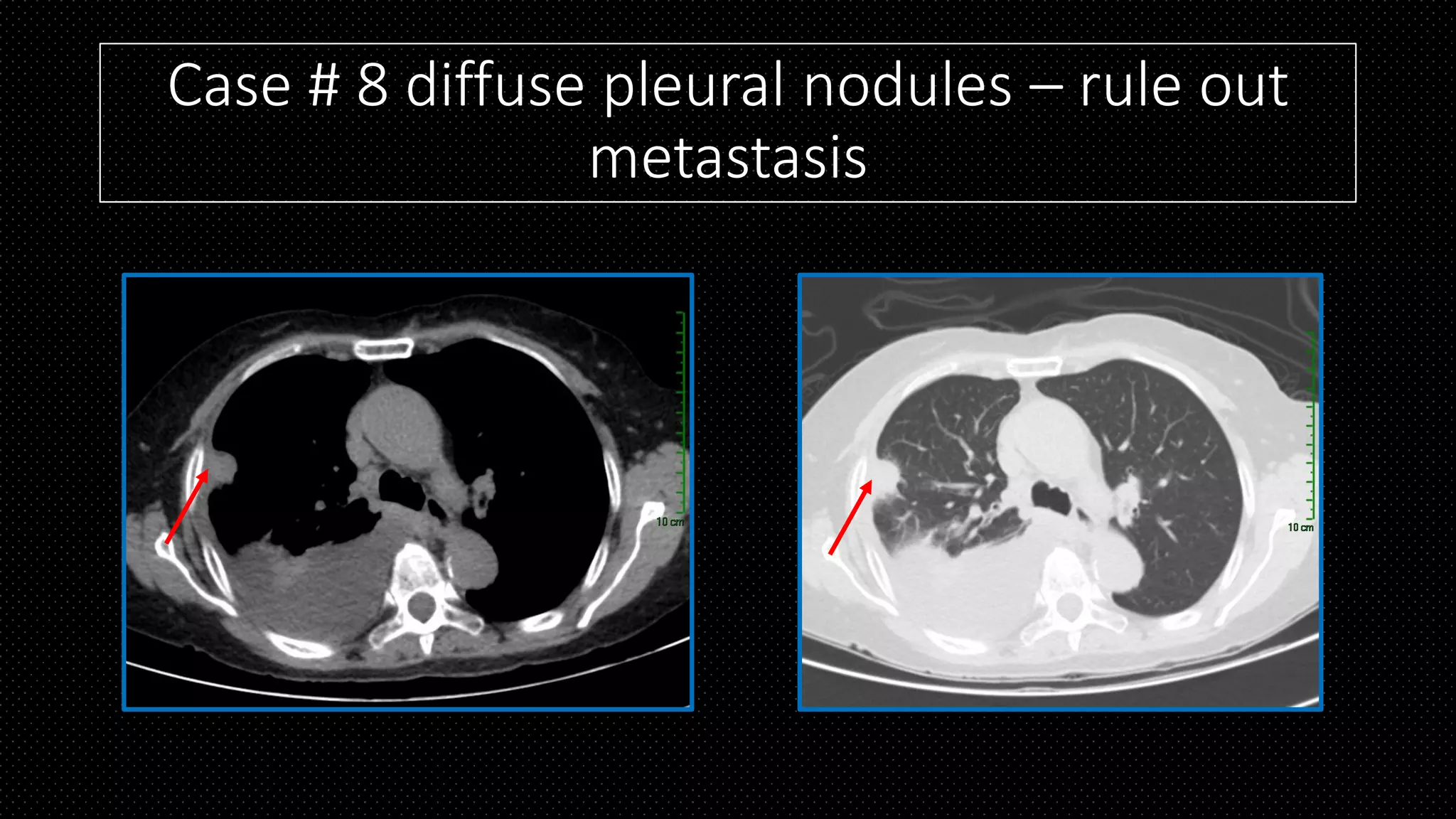
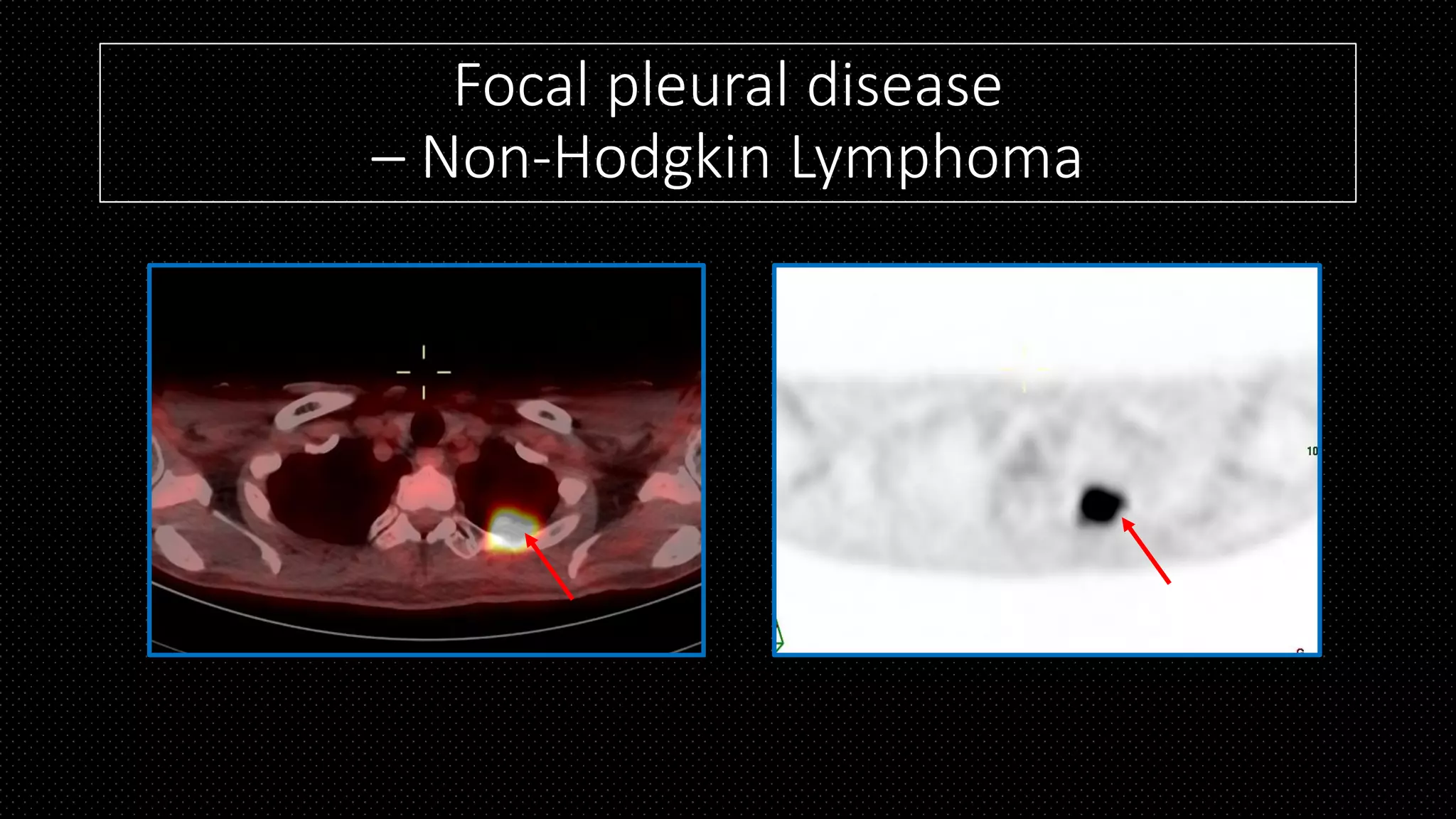
The document discusses emerging updates and advances in pleural diseases, covering anatomy, various types of effusions, and the differentiation between empyema and abscess. It highlights diagnostic approaches using ultrasound, CT scans, and FDG-PET for conditions like tuberculosis, mesothelioma, and metastasis. Additionally, it examines patterns of pleural calcifications, the impact of asbestos exposure, and various case studies to illustrate key points.