Downloaded 17 times

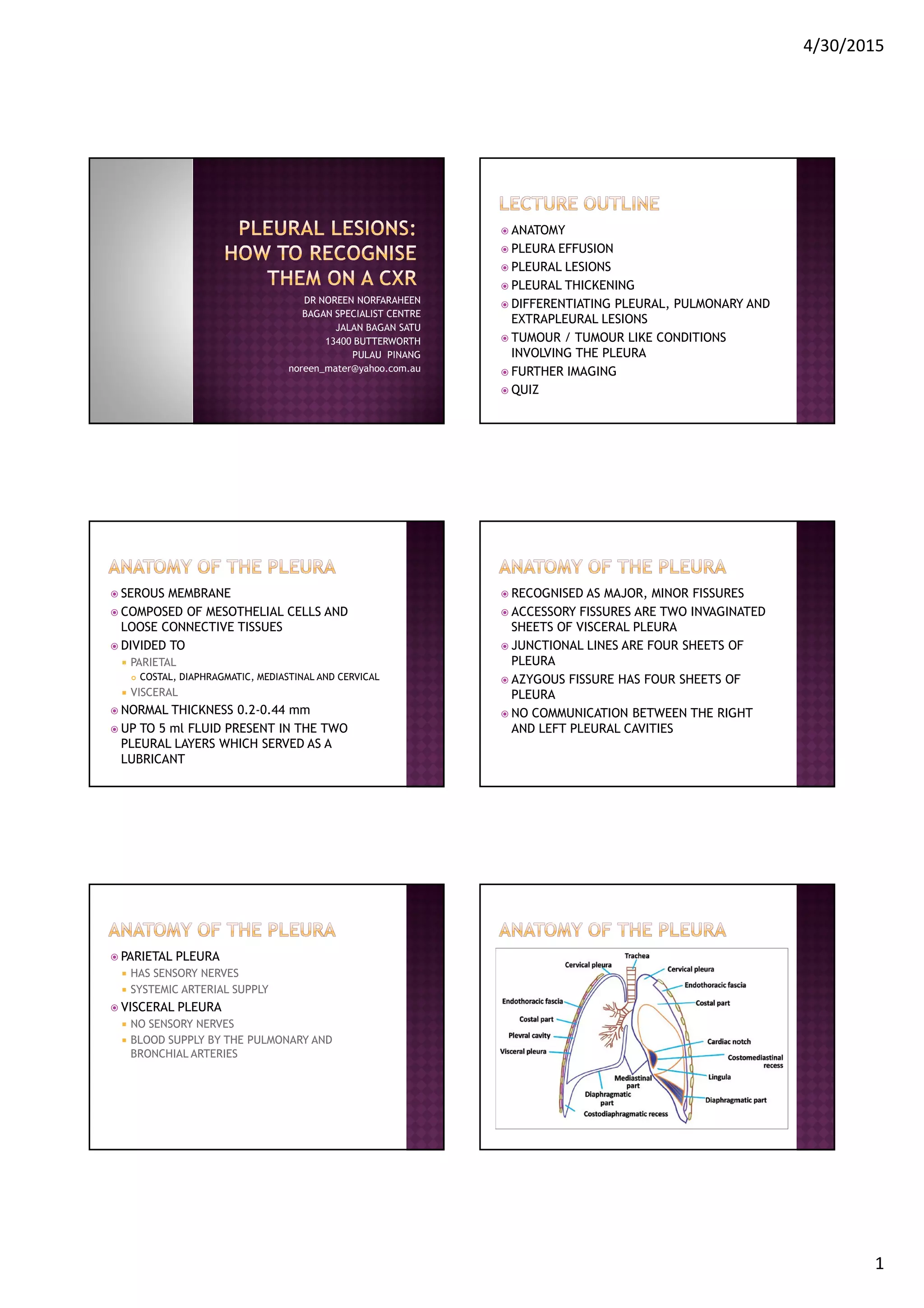



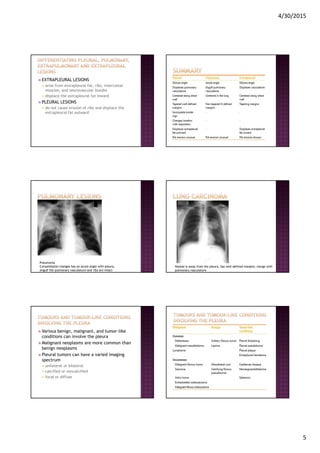




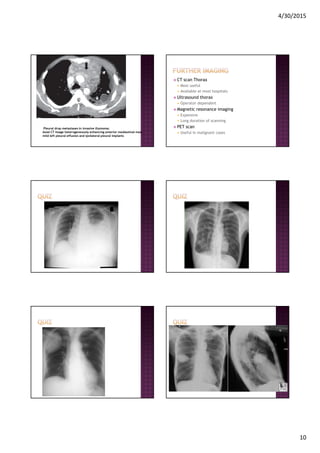


This document provides information on pleural effusions and pleural lesions. It discusses the anatomy and physiology of the pleura, as well as common causes of pleural effusions such as congestive heart failure, pneumonia, and cancer. Various pleural lesions are also described, including pleural thickening, empyema, fibrous tumors, mesothelioma, metastases, and lymphoma. Imaging features of these conditions on chest x-ray and CT are presented, along with appropriate differential diagnoses and diagnostic workup.





































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)














