Downloaded 19 times
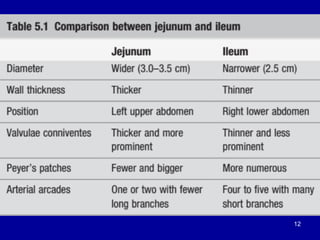
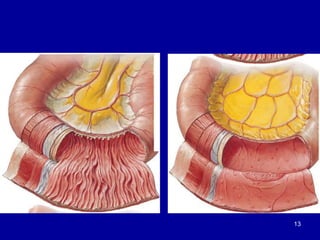
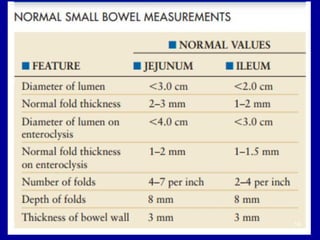
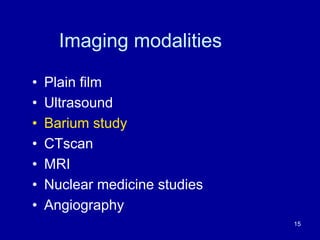



The document provides an overview of the radiologic anatomy of the mesenteric small bowel. It discusses the embryology and development of the small bowel. The anatomy of the small bowel is then described, including its length, attachments, blood supply, and lymphatic drainage. Various imaging modalities for evaluating the small bowel are reviewed, such as plain films, ultrasound, barium studies, CT, MRI, and nuclear medicine scans. Specific techniques for barium studies, enteroclysis, CT enterography, and MRI enterography are outlined.










































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
