NDCT Rules, 2019: An Overview | New Drugs and Clinical Trial Rules 2019
Bmi 403
1. SMU-DDE-Assignments-Scheme of Evaluation
Q.No Criteria Marks Total
Marks
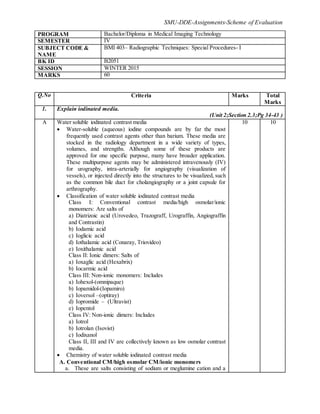
1. Explain iodinated media.
(Unit 2;Section 2.3;Pg 34-43 )
A Water soluble iodinated contrast media
Water-soluble (aqueous) iodine compounds are by far the most
frequently used contrast agents other than barium. These media are
stocked in the radiology department in a wide variety of types,
volumes, and strengths. Although some of these products are
approved for one specific purpose, many have broader application.
These multipurpose agents may be administered intravenously (IV)
for urography, intra-arterially for angiography (visualization of
vessels), or injected directly into the structures to be visualized, such
as the common bile duct for cholangiography or a joint capsule for
arthrography.
Classification of water soluble iodinated contrast media
Class I: Conventional contrast media/high osmolar/ionic
monomers: Are salts of
a) Diatrizoic acid (Urovedeo, Trazograff, Urograffin, Angiograffin
and Contrastin)
b) Iodamic acid
c) Ioglicic acid
d) Iothalamic acid (Conaray, Triovideo)
e) Ioxithalamic acid
Class II: Ionic dimers: Salts of
a) Ioxaglic acid (Hexabrix)
b) Iocarmic acid
Class III: Non-ionic monomers: Includes
a) Iohexol-(omnipaque)
b) Iopamidol-(Iopamiro)
c) Ioversol –(optiray)
d) Iopromide – (Ultravist)
e) Iopentol
Class IV: Non-ionic dimers: Includes
a) Iotrol
b) Iotrolan (Isovist)
c) Iodixanol
Class II, III and IV are collectively known as low osmolar contrast
media.
Chemistry of water soluble iodinated contrast media
A. Conventional CM/high osmolar CM/ionic monomers
a. These are salts consisting of sodium or meglumine cation and a
10 10
PROGRAM Bachelor/Diploma in Medical Imaging Technology
SEMESTER IV
SUBJECT CODE &
NAME
BMI 403– Radiographic Techniques: Special Procedures- I
BK ID B2051
SESSION WINTER 2015
MARKS 60
2. SMU-DDE-Assignments-Scheme of Evaluation
triodinated benzoate anion.
b. Anions consisting of a benzoic acid molecule with three atoms of
iodine firmly attached at C2, C4 and C6.
c. The C3 and C5 are connected to radicals CR3 and R5, which are
amines E-NH2, and greatly reduce toxicity and increase
solubility of the molecules.
d. Iodine particle ratio is 3:2.
e. Sodium or meglumine act as cations.
B. Lowosmolar contrast media: Low osmolar contrast media is
classified into ionic dimers, non ionic monomers and non ionic dimers.
Now, let us discuss these types in detail.
Ionic dimers
a) Two benzene rings (each with three iodine atoms) are linked by a
bridge to form a large compound. E.g. Hexabrix.
b) This group carries only one carboxyl group. So known as monoacid
dimmers.
c) Iodine particles ratio is 6:2.
Non-ionic monomer (NIM)
a) Carboxyl group (-COOH) at C-1, of monomeric salts is replaced by
a non-ionizing radical and CONH2 producing iodine: particle ratio
of 3:1.
b) Metrizamide (Amipaque) was the earliest non-ionic monomer and
proved as an excellent contrast media but was very expensive,
impossible to autoclave and unstable in solution, so second
generation of NIM were included later such as:
a) Iohexol (omnipaque)
b) Iopamidol (Iopamiro)
c) Ioversol (optiray)
d) Iopromide (Ultravist)
c) Iodine: particle ratio is 3:1
Non-Ionic dimers
Iodine: Particle ratio is 6:1
E.g.: Iotrol; Iotrolan (Isovist).
Ionic and non-ionic contrast media available in India
A. Ionic contrast media available in India
B. Non-ionic contrast media available in India
2. Discuss the various types of contrast reactions of contrast media.
(Unit 3;Section 3.2;Pg 37-41)
A Contrast reactions are classified into following types:
Reactions unrelated to contrast media
Hyper osmolarity
Chemotoxic actions
Immunological toxicity
2 10
Reactions unrelated to contrast media
The various reactions related to contrast media are as follows:
a) Pyrogenic (unsterile injection): Management is through
i) Stop injection
ii) Reassure the patient
iii) Blanket
2+2+2+2
3. SMU-DDE-Assignments-Scheme of Evaluation
iv) Once chills occur-change the syringe, contrast and scalp vein set.
v) No need for medication.
b) Vasovagal especially in anxious or psychosomatic patient.
c) Hypertensive attacks in patient with pheochromocytoma.
d) Excessive dehydration, hypoglycaemia.
Hyper osmolarity
This is due to the high osmolarity of contrast media than plasma. It is
more with conventional contrast media. These reactions include:
a) Erythrocyte damage
b) Capillary endothelial damage
c) Vasodilatation
d) Hypervolemia
e) Cardiovascular effects
f) Vascular pain
g) Distrubance of BBB
h) Thrombosis and thrombophlebitis
Chemotoxic actions
Chemotoxic effects are usually due to the cations, especially Na+. The
effects are seen in
a) Neurons
b) Myocardial cells
c) Capillary endothelium
d) RBC
e) Kidney
Immunological toxicity
Immunological (allergic) toxicity mechanisms are as follows:
a) Deactivation of angiotensin converting enzyme. Incidence of adverse
contrast media reactions to intra-arterial injection is about 1/3 of
incidence following intravenous injection because the latter
stimulate release of vasoactive substances from mast cells or
deactivates ACE in lung. ACE deactivates bradykinin, the
concentration of which rises with IV injection of contrast media.
b) Due to damage to the endothelium which initiates the activation
system, which in turn may be responsible for many adverse
anaphylactoid reactions.
c) Activation of complement, kinins, coagulation and fibrinolytic
systems.
d) Inhibition of cholinesterase with consequent vagal over stimulation –
acetylcholine release – collapse, bradycardia, bronchospasm.
e) Release of vasoactive substances like histamine, bradykinin,
serotonin.
3. Explain barium swallow radiographic examination of upper gastrointestinal tract.
(Unit 4;Section 4.3;Pg 61-65)
A
Barium swallow is a radiographic examination of the upper
gastrointestinal tract, specifically the pharynx (back of mouth and throat)
and the esophagus (a hollow tube of muscle extending from below the
1 10
4. SMU-DDE-Assignments-Scheme of Evaluation
tongue to the stomach).
Indications of barium swallow:
1. Dysphagia and obstruction.
2. Pain during swallowing.
3. Assessment of mediastinal masses.
4. Assessment of left atrial enlargement.
5. Pre-operative assessment of carcinoma bronchus and oesophagus.
6. Motility disorders of oesophagus, e.g.: Achalasia and diffuse
oesophageal spasm, scleroderma.
7. Assessment of site of perforation.
8. Zenker’s diverticulum and cricoid webs. In these cases water
soluble contrast media are used. E.g.: Gastrograffin or dionosil
aqueous.
Contraindications of barium swallow: Tracheo oesophageal fistula
and perforation.
2
Contrast media: Contrast media used in barium swallow are as follows:
a) 100% barium sulphate paste.
b) 80% barium sulphate suspension.
c) 30% barium sulphate suspension for high kV technique.
d) 200-250% high density, low viscosity for double contrast study.
1
Preparation: Patient undergoing barium swallow procedure should be
prepared in following ways:
a. Patient should not eat or drink for at least 6 hours before
examination. Patients who are undergoing a routine study during a
morning session are usually told to fast overnight.
b. As cigarette smoking may interfere with optimum coating of the
mucosa, patients should restrain from smoking.
c. As prolonged fasting is harmful for patients with diabetes, early
morning appointment should be arranged.
d. In patients with gastric outlet obstruction, prolonged fasting or
intravenous metaclopramide and sometimes nasogastric incubations
and aspiration of the contents may be necessary.
2
Technique: Explanation of single and double contrast barium
swallow study
Specific conditions of barium swallow
4
4. Discuss single and double contrast barium enema in detail.
(Unit 8;Section 8.3;Pg 107-111)
5. SMU-DDE-Assignments-Scheme of Evaluation
A Single Contrast Barium Enema (SCBE)
Indications:
Unco-operative, very debiliatated or immobile patient.
Evaluation of acute obstruction or volvulus.
Reduction of intus susception.
Show configuration of colon.
Where only gross pathology is to be excluded.
Contra-indications:
Allergy to barium suspension.
Risk of perforation.
Peritonitis.
Suspicion of acute/fulminating ulcerative colitis.
Following a recent deep biopsy.
Procedure: Barium suspension - Low density (to promote see through
effect with a high kV or compression) 15% to 20% w/v. Tube is placed
in the rectum with the patient in left lateral position. The height of the
enema should not be more than 1 meter above the table top. In case there
is gas in the rectum, the patient is kept supine and infusion is started.
Otherwise the patient is kept in left lateral position. As soon as the entire
rectum is full, the tube is clamped and a lateral view is taken. Then the
patient is put prone and with the infusion running, the frontal view film
of the rectum is exposed. In the prone position, pelvis tilts forward,
sacrum, lies parallel to the film and foreshortening of rectum is
prevented. The patient is kept prone with right side down oblique
position. This position helps in the opening up the curve of rectosigmoid
junction. Spot views of rectosigmoid junctions with barium flowing are
taken.
Now, the patient is kept prone oblique with the left side down. Splenic
flexure opens out and spot view of splenic flexure is taken. As barium
flows towards hepatic flexure, patient is turned right side down oblique
and spot films of hepatic flexure are taken. With the continuous flow of
barium caecum fills up. As soon as the reflux across ileocaecal junction
takes place, the tube is clamped and ileocaecal spot films are exposed. A
full film is now exposed to show entire colon. After evacuation, mucosal
relief film is exposed. Polyposis and diverticulosis can be better
visualized on post-evacuation films.
5 10
Double Contrast Barium Enema (DCBE)
Preliminary films: Plain radiograph of the abdomen is essential and
helps in assessing any abnormalities of gas filled bowel loops. In the
presence of residual fecal matter, double contrast examination should be
cancelled. In many centers, barium enemas are performed after an
excretory urogram. This not only reduces the time of hospitalization but
also gives the relationship of the urinary system to the colon. It also
helps in visualization of the bladder in frontal and lateral projections and
this permits the study of the space betweend bladder and rectrum.
Indications:
5
6. SMU-DDE-Assignments-Scheme of Evaluation
1) Preferred method for routine examination.
2) High risk patients – rectal bleeding, previous H/o(history of)
carcinoma or polyp, family H/o colorectal cancer or polyposis.
3) Demonstration of sinuses or fistulas.
4) Patient with severe diverticulosis, polposis or diarrhoea.
5) Presence of obstruction.
6) Reduction of an intus susception.
Contraindications:
1) Allergy to barium suspension.
2) Peritonitis.
3) Acute or fulminating inflammatory colon disease.
4) Debilitated, unconscious, inability to co-operate.
5) History of recent rectal/colonic biopsy.
Procedure: Barium suspension-high density (slower flowing, better
coating) 75% to 95% w/v.The patient is in prone position with left side
down oblique and high density, low viscosity barium suspension is
allowed to flow upto splenic flexure. Now, air is introduced with patient
prone. Air should push the barium column and never pass beyond the
column. The role of IV muscle relaxant before or after the double
contrast barium study had found to have no effect on the mucosal
coating. Frontal view of rectrum is taken in the prone position and then
the patient is turned left lateral to take the lateral view. Then oblique
right side down view for rectosigmoid junction is taken. The patient is
taken back in a prone position with right side dependent and air is
pumped into left sided colon. Once barium comes into transverse colon
turn the patient left side up – barium enters right sided colon and reaches
the ileocaecal junction. Now with the right side up, more air is pumped
till air outlines the ileocaecal junction. Now with the right side up, more
air is pumped till air outlines the ileocaecal junction. Take spot films for
flexures and ileocaecal junction. Now proceed with full films in supine,
both decubitus and erect as required.
Advantages of DCBE:
a) Better surface details.
b) Surface lesions can be demonstrated to the best effect.
c) The easy unraveling of the colon as it is possible to look through
loops.
Disadvantages DCBE:
a) Difficult in uncooperative patients.
b) Fistulae/sinuses can be missed.
c) Effacement of submucosal detail of the colon and overlooking of
annular/polypoid lesion is possible.
5. Explain intravenous urogrogram and retrograde pyeloureterography.
(Units 9 &12;Sections 9.3 and 12.3)
7. SMU-DDE-Assignments-Scheme of Evaluation
A Intravenous Urogram
Intravenous urogram is the radiographic examination of urinary tract
including renal parenchyma, calyces and pelvis after intravenous
injection of contrast media.
Indications, contraindications and risk factors
Contrast media and mode of injection
Patient preparation
Procedure
a) The patient is placed in supine position with pelvis at cathode side of
the tube.
b) A support is placed under patient’s knees to reduce lordotic
curvature of lumbosacral spine and provide comfort.
c) A scout film is taken including the kidneys, ureters, bladder and
urethral regions on a large size film.
d) Contrast media is injected intravenously into a prominent vein in the
arm. Test injection of 1 ml of contrast is given and patient is
observed for 1 min to look for any contrast reactions. Then the rest
of the contrast is rapidly injected within 30-60 seconds.
e) Cortical nephrogram is seen within 20 seconds of contrast injection.
This depicts the renal parenchyma opacified by contrast. The
nephrogram is made up of cortical phase due to vascular filling and a
tubular phase due to contrast within the lumen of renal tubule.
Density of the nephrogram depends on the dose of contrast and the
peak plasma level.
f) The appearance of pyelogram (contrast in calyces) is seen 2 minutes
after contrast injection. During its transit, it may be concentrated as
much as 50 times producing a dense pyelogram.
g) If a kidney fails to excrete detectable amount of contrast media into
collecting system, it is termed as non-visualising kidney. This does
not necessarily mean that the kidney is not functioning.
Filming technique: Low kV (65-75) high mA (600-1000) and short
exposure should be used to get optimum image contrast. Standard films
taken are as follows:
1. Plain x-ray KUB/Scout film – 14" x 17"
2. 1 minute film – 10" x 12"
3. 5 minute film – 10" x12"
4. 10 minute film – 15" x 12"
5. 15 minute film – 15" x 12"
6. 35 minute film – 14" x 17"
7. Post-void film – 10" x 8"
Special films in IVU
5 10
8. SMU-DDE-Assignments-Scheme of Evaluation
Retrograde Pyelogram is a urologic procedure where the physician
injects contrast into the ureter in order to visualize the ureter and
kidney. The flow of contrast (up from the bladder to the kidney) is
opposite the usual flow of urine, hence the retrograde name.
Indications, contraindications and contract medium
Procedure
1. Patient preparation: Bowel preparation with cathartics is not
routinely performed.
2. Preliminary film: Full length supine AP abdomen before the
examination is started.
3. Anesthesia: May be performed under local anesthesia although
general anesthesia is often required. Sterile precautions are
mandatory.
4. Technique: In the operating theatre the surgeon catheterizes the
ureter via a cystoscope and advances the ureteric catheter to the
desired level. Contrast medium is injected under fluoroscopic
control and spot films are exposed.
Films: Using the under couch tube supine PA film of the kidney and
both 35 anterior obliques of the kidneys are taken. Low kVp (65-75
kVp) technique is used to visualize calculi and contrast medium. If there
is pelvi-ureteric junction obstruction, the contrast medium in the pelvis is
aspirated. The films are examined and if satisfactory, the catheter is
withdrawn, first to 10 cm below the renal pelvis and then to lie above the
ureteric orifice. About 2 ml of contrast medium is injected at each of
these levels and films are taken.
After care and complications
5
6. Describe sialography in detail.
(Unit 14;Section 14.3;Pg 183-185)
A Theatre radiography plays a significant role in the delivery of surgical
services. The following settings are typical examples where the
radiographer is required.
a) Non-trauma corrective orthopaedic surgery
b) Trauma orthopaedic surgery
c) Interventional urology
d) Operative cholangiography
e) Specialized hysterosalpinography procedures
f) Emergency peripheral vascular procedures.
Liaison: The radiographer should contact the theatre superintendent on
arrival in the theatre, and maintain a close liaison with all persons
performing the operation. Radiographers should have a working
knowledge of the duties of each person in the operating theatre, and
check on the specific requirements of the surgeon who is operating.
10 10
9. SMU-DDE-Assignments-Scheme of Evaluation
Personal preparation: In many modern theatre suites it is normal for x-
ray equipment and darkroom processing facilities to be housed within
the complex. The first thing that each radiographer must be concerned
with is their own personal preparation before entering an aseptic
controlled area. Uniform and any jewelry is removed and replaced by
theatre wear. The hair is completely covered with a disposable hat, and
theatre shoes or boots worn. Special attention is then made to washing
the hands, using soap, paying particular attention to the nails with a
scrubbing brush. A face mask is put on. If the skin has an abrasion, this
should be covered with a clean plaster. A film monitoring badge is
pinned to the theatre garment.
Equipment: Portable or mobile x-ray units are selected, depending on
the requirement of the radiographic procedure. This may mean a high-
powered mobile x-ray unit for abdominal radiography, or a mobile
image intensifier for screening of orthopaedic procedures, such as hip
pinning. Before a unit is removed from its store, it is switched on and
tested. It is then disconnected from the electrical supply and dusted with
a dry absorbent cloth to remove superficial dust. Using a cloth moistened
with a suitable antiseptic solution in alcohol base, all parts of the mobile
unit are cleaned with special attention to cables and wheels. After the
unit has dried, it is transferred to the theatre, tested again, and if
functioning positioned ready for use. Exposure parameters are then
adjusted to those required for screening or image recording on a film.
The image intensifier housing or x-ray tube housing is covered with a
sterile towel by staffs that are scrubbed for the operation.
Darkroom facilities: Processing equipment should be switched on and
tested. Adequate levels of replenisher solutions should be prepared if
required and a supply of cassettes and films made available for use.
Accessory equipment: Cassette holders, stationary grids, cassette
tunnels or serial changer devices should be cleaned and checked if
required. An operating theatre table with an adjustable cassette tray
should be checked for movement, and the radiographer should be
familiar with the function and be able to position cassettes when
requested. Contrast media, if required, should also be supplied to the
theatre staff.
Radiation protection: Radiation protection is the responsibility of the
radiographer operating the x-ray equipment. The radiographer should
ensure that film monitoring badges and lead rubber aprons are worn
where necessary, and staffs are sent out of theatre if not required during
exposure. Use of the inverse square law with staff standing at the
maximum distance from the source of radiation, and outside the path of
the radiation field, should be made during exposure. The radiation field
should be collimated to the size of the film or intensifier and cassette
support devices should be used to hold cassettes. The radiographer
should use the fastest film/screen combination consistent with the
examination and type of processing to reduce radiation dose. Records
should be kept of exposure times when screening is employed. The
10. SMU-DDE-Assignments-Scheme of Evaluation
radiographer must give clear instructions to staff before exposures are
made regarding their role to reduce the risk of accidental exposure.
Sterile areas: The radiographer should avoid the contamination of
sterile areas. Ideally, equipment should be positioned before any sterile
towels are placed in position, and care should be exercised not to touch
sterile areas when positioning cassettes or moving equipment during the
operation.
*A-Answer
Note –Please provide keywords, short answer,specific terms, specific examples (wherever necessary)
***********