COOL LLC
BUSINESS PLAN
7/8/2013
Legal Page
Confidentiality Agreement
The undersigned reader acknowledges that the information provided by _______________ in this business plan is confidential; therefore, reader agrees not to disclose it without the express written permission of _______________.
It is acknowledged by reader that information to be furnished in this business plan is in all respects confidential in nature, other than information which is in the public domain through other means and that any disclosure or use of same by reader, may cause serious harm or damage to _______________.
Upon request, this document is to be immediately returned to _______________.
___________________
Signature
___________________
Name (typed or printed)
___________________
Date
This is a business plan. It does not imply an offering of securities.
Table of Contents
Legal Page2
Executive Summary5
Business Description5
Mission5
Vision5
Values5
Proposed Location6
Description of Services6
Market Analysis6
Target Population6
Market Trends8
Market Needs9
Strategy and Implementation9
Marketing Strategy9
Referral Strategy10
Payors Strategy10
ORGANIZATION AND MANAGEMENT10
Legal Form of Organization10
Management Summary10
Organizational Structure11
FINANCIAL ANALYSIS134
Capital Requirements13
Financial Indicators145
Appendix146
References202
Executive Summary
This business plan describes the roadmap to sustained profitability for COOL, a private for profit District Of Columbia Company. As a private behavioral health services provider, we are committed to providing a comprehensive array of clinical services and treatments to individuals diagnosed with mental illness and substance abuse disorders. We understand the market and have developed vibrant plans to penetrate and increase our market share through the marketing and promotion of the level of services identified in this business plan. Our financial analysis is conservative in its projections and indicates a path to profitability that we are committed to executing while remaining flexible to continue to take advantage of opportunities presented by the market.Business Description
COOL is a multidisciplinary behavioral health services provider committed to the provision of comprehensive consumer driven services In addition, our target population will include individuals with mental health and co-occurring disorders. We are dedicated to providing quality and cost effective treatments/services that are undergirded by culturally competent best practices in the field of behavioral mental health. The aforementioned population will be the focus of our certified Free Standing Mental Health Clinic (FSMHC). COOL as part of our future development will consider becoming a CSA. Mission
The mission of COOL is to provide excellent comprehensive, consumer driven, and quality mental health services for individuals and families in the community in order to enhance their quality of life. It is part of our missi.
1. COOL LLC
BUSINESS PLAN
7/8/2013
Legal Page
Confidentiality Agreement
The undersigned reader acknowledges that the information
provided by _______________ in this business plan is
confidential; therefore, reader agrees not to disclose it without
the express written permission of _______________.
It is acknowledged by reader that information to be furnished in
this business plan is in all respects confidential in nature, other
than information which is in the public domain through other
means and that any disclosure or use of same by reader, may
cause serious harm or damage to _______________.
Upon request, this document is to be immediately returned to
_______________.
___________________
Signature
___________________
Name (typed or printed)
___________________
Date
This is a business plan. It does not imply an offering of
securities.
Table of Contents
2. Legal Page2
Executive Summary5
Business Description5
Mission5
Vision5
Values5
Proposed Location6
Description of Services6
Market Analysis6
Target Population6
Market Trends8
Market Needs9
Strategy and Implementation9
Marketing Strategy9
Referral Strategy10
Payors Strategy10
ORGANIZATION AND MANAGEMENT10
Legal Form of Organization10
Management Summary10
Organizational Structure11
FINANCIAL ANALYSIS134
Capital Requirements13
Financial Indicators145
Appendix146
References202
Executive Summary
This business plan describes the roadmap to sustained
profitability for COOL, a private for profit District Of
3. Columbia Company. As a private behavioral health services
provider, we are committed to providing a comprehensive array
of clinical services and treatments to individuals diagnosed with
mental illness and substance abuse disorders. We understand the
market and have developed vibrant plans to penetrate and
increase our market share through the marketing and promotion
of the level of services identified in this business plan. Our
financial analysis is conservative in its projections and indicates
a path to profitability that we are committed to executing while
remaining flexible to continue to take advantage of
opportunities presented by the market.Business Description
COOL is a multidisciplinary behavioral health services provider
committed to the provision of comprehensive consumer driven
services In addition, our target population will include
individuals with mental health and co-occurring disorders. We
are dedicated to providing quality and cost effective
treatments/services that are undergirded by culturally competent
best practices in the field of behavioral mental health. The
aforementioned population will be the focus of our certified
Free Standing Mental Health Clinic (FSMHC). COOL as part of
our future development will consider becoming a CSA. Mission
The mission of COOL is to provide excellent comprehensive,
consumer driven, and quality mental health services for
individuals and families in the community in order to enhance
their quality of life. It is part of our mission to promote active
recovery models and be accountable to our consumers by
fostering positive customer relationship. Vision
To be the leading industry provider of mental health services in
the Region.Values
Quality: Our services will be cost-effective and incorporate
high standards, cultural competence, best practices and
consumer satisfaction as part of its outcome measures. Our
board of directors, executive management team, support staff
and clinicians are committed to professional integrity, ethical
business practices and objectivity.
Respect: We are committed to treating all persons with respect
4. and dignity. Each individual is valued for their abilities and
contributions that they bring to the therapeutic relationship.
Caring: We will foster a spirit of genuine partnership with our
clients/consumers, family members, providers and others
through unconditional positive regard for their
concerns.Proposed Location
As a for-profit company which will be located in the SE
quadrant of the District of Columbia., with our initial focus
being residence of Ward 7. The future plan is to expand offices
within other segments of the District of Columbia. Description
of Services
COOOOL is organized to provide a wide array of quality
behavioral mental health and substance abuse/addiction
treatments and services to the population of individuals
diagnosed with mental illnesses, substance abuse and co-
occuring disorders.
FSMHC will include:
· Medication Management
· Psychopharmacology
· Psychotherapy
· Substance abuse/Addiction
· Group therapy for substance abuse
· Integrated mental health/primary care services via MOU
agreement with a primary care facility, Unity or FQHCF
· Family Therapy
· Family Conference
· Complete Psychological Testing
·
All new and expanded services will be consistent with
documented service needs of the target populations and be
clinically and fiscally viable.Market AnalysisTarget Population
The target population comprises mostly of adults with a mental
illness, substance abuse problem, and co-occuring disorder. The
primary referral sources will consist of Access Helpline,
CSOSA, CSA’s, MCO’s, APRA, family members, and the
general community.
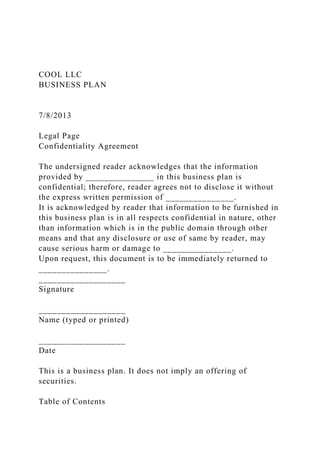
5. COOL PROGRAM (CONSUMERS SERVED)
While the graph show an initial consumer base of 300, which
reflects 3-4 months from start up, the 2nd year is expected to
grow at a pace of 1/3 trend from the initial 3 months. The 3rd
year is expected to have a 25% increase in volume of
consumers.
6. The objectives of COOL in targeting our services to these
populations are:
· Expand access and coverage to all eligible individuals in the
population
· Provide positive treatment and service experience to
consumers.
· Identify and develop strategic alliances with the network of
community providers to better serve the individuals in the target
population.
· Become a premier provider of mental health services in the
region. Market Trends
The local market, just as the national market for behavioral
health services, is highly segmented and competitive. Currently,
the national trends impacting service delivery are: increased use
of Medicaid managed care organizations (MCOs), contracts with
health maintenance organizations (HMOs), and preferred
provider organizations (PPOs). The other national trends likely
to impact service delivery are the recently passed Affordable
Care Act of 2010 and the Republican Party- controlled House of
Representatives’ proposal to reform Medicaid and Medicare.
These trends will most certainly affect local DC market
although the form and extent of the likely effects are currently
unknown.
Locally, the major trend impacting public behavioral health
delivery is the 2009 privatization of services. In 2009, DMH
ceased to be the dominant, primary provider of public
behavioral health services in DC. It certified private providers
to deliver its MHRS programs to DC citizens diagnosed with
mental/emotional illnesses. These changes, coupled with the
increasing use of MCOs , are impacting not only the range of
services and financing of public mental health in DC but also
the issue of access, reach and effectiveness of public behavioral
health programs.
The DC local market for behavioral health services is alive and
well. It boasts abundant supply of providers that include
psychiatric hospitals, community service agencies (CSAs),
7. residential crisis and non-crisis facilities, and outpatient
multidisciplinary group practices that vary from private group
practices to solo practitioners. Our competitors are all of these
providers, with the CSAs being our direct competition and
FSCMH clinics.
We plan to differentiate ourselves not only by being customer-
driven in terms of providing superior customer service but also
by focusing on our niche market. We will vigorously market our
services through the network of private and public providers,
and directly to potential customers through various media
outlets. Our differentiation strategies equally include
developing reputation for providing quality services,
demonstrating respect for our clients, responding promptly to
the needs of our referral sources, and making
psychopharmacologic services available to our consumers.
Market Needs
The need for behavioral health services in DC for our target
population is illuminated by the following statistics:Strategy
and Implementation
COOL will focus its market activities initially in the SE
quadrants of the city with projections to expand in other DC
wards for the target populations, however more targeted
outreach will occur in quadrants with the largest populations of
potential consumers. Our services will include the FSCMH
services of diagnosis and assessment, psychopharmacology,
psychotherapy, substance abuse/addiction services, family
therapy, family conferences, and complete psychological
testing.
Our customers are consumers belonging to the target population
who are referred to us by DMH, CSOSA, CFSA, DYRS, MCO’s.
and its affiliate agencies (public and private), self-referred
individuals, couples and/or families, and referrals from area
psychiatric wards and PPOs. We anticipate that adults will
constitute about 90% of our consumers, and
children/adolescents about 10% initially.
8. Marketing Strategy
Targeting our marketing activities in a strategic manner will be
critical to growth. Strategies will include:
· Emphasizing our customer-driven, quality, and innovative
services
· Focusing on CSOSA, DMH, CFSA, CSA’s and the general
population for referrals (expectation is that 70% of our initial
client populations will be referrals from DMH’s access
helpline).
· Building strategic business relationships with other private
providers in the community
· Increasing our market penetration of the target population
Our focus will be on increasing visibility and creating a unique
brand. We will engage in the following promotion activities:
· Advertise in local newspapers to promote our services and
interventions
· Create logo, brochures, and business cards to promote the
agency.
· Host an open house
· Collaborate and network with various providers network
groups in DC and its Metropolitan area.
· Ensure follow-ups with our referral sources through the use of
phone calls, letters and email as necessary
· Organize and offer informational workshops and seminars to
the public
· Visit other providers and referral sources at their sites to
provide information and awareness about our services and
interventions.
· Develop public service announcements
· Host referral breakfast and lunch
Referral Strategy
Our referral strategy will target potential purchasers and seek
referrals from the following sources:
· DMH and its public/private affiliates
· PPOs and MCOs
9. · Local private and public psychiatric hospitals
· Medical groups
· CFSA and DYRS
· Employers and EAPs
· Private individuals
Payors Strategy
Our pricing for services and interventions will be market-driven
and based on the DMH for the services we are certified to
provide. Our fee structure will also reflect other payors’
(Medicaid/Medicare, MCOs, PPOs, Private insurance, Self paid
etc.) fee schedule. In view of the structured nature of the prices
that can be billed to our customers, it becomes imperative that
we monitor and control costs in order to operate profitably.
Thus, staffing will be based on level of clinical needs.
ORGANIZATION AND MANAGEMENTLegal Form of
Organization
Cool is a privately incorporated company in the District of
Columbia. The company was founded by a group of individuals
with over 45 years of combined experience in behavioral health
and executive management.Management Summary
Cool LLC Management Board, is made up of the followings:
Carroll Parks, Chairman
Guillaume Kengni Vice Chairman
Michele Mba, Chief Executive Officer
Brian Fallon, Chief Financial Officer
The day-to-day management of COOL, LLC. operations will be
under the President/CEO, Michele Mba . Ms. Michele Mba has
over 6 years of experience both as administrator and clinician in
the behavioral health industry. A management team consisting
of senior level managers will incorporate the programs and
services within the operations of COOL. The policy and practice
guidelines will reside with the Board of Directors. The
President/CEO and the Medical Director will ensure that the
company maintains a fidelity to best organizational and clinical
practices. Organizational Structure
10. The company will be managed by the President. A Medical
Director will assist the President in all clinical decision-
making. Clinical services will be provided to our consumers by
teams of behavioral health professionals consisting of
psychiatrists, nurses, psychologists, social workers, mental
health therapists, and certified addiction counselors. The
company’s support staff will consist of a Chief Financial
Officer (CFO), a Receptionist, a Billing Staff and a medical
record personel. A QA committee made up of the company’s
staff , one consumer, and chaired by the QA Director will be
constituted and assigned the task of developing a plan to
implement and integrate continuous quality improvement. A
customer relations committee will be formed to develop,
formulate and implement activities to enhance level of
satisfaction among all consumers.
Organization Chart
Some of the company’s staff will be hired as salaried employees
and others as contract staff. The salaried employees are
expected to work 40 hours weekly and will be paid every two
weeks. The contract staff will be paid for the hours of services
billed based on contracted rate for each service. Contract staff
will be paid once monthly. FINANCIAL ANALYSISCapital
Requirements
The following assumptions undergird the company’s financial
projections:
· We will commence operation with initial enrollment of at least
80 adult consumers in November of, 2013.
· The wrap of staffing and consumers will be operational by
December of 2013
· The billing for services rendered will maintain a 30 day
adjudication cycle based upon Medicaid usual payment and
processing. COOL anticipate 98% clean rate for claims and a
less than 45 day aging on receivables.
· The company will achieve an annualized base of consumers of
11. 900 by 2nd year, then a 15% increase in volume of consumers
for years 3-5. The 5th year base of consumers will be 1400
active consumers.
The business will require initial start-up capital. The start-up
capital needed is estimated at about $150,000. Please see the
Start-up Requirements and Start-up Funding tables below. This
amount will be funded through direct cash infusion by the
company’s president and CCS ownership.
Start-up Requirements
Requirements
Start-up Expenses
Legal
$5000
Stationery etc.
$2,000
Insurance
$8,000
Rent
$15,000
Computer/software
$10,000
Office Furniture
$15,000
Telephone, copier, fax
$5,000
Staff/consultant
$85,000
Misc.
$5,000
12. Total Start-up Expenses(investor)
$150,000
Start-up Assets
Cash Required(Officers)
$25,000
Other Current Assets
$0
Long-term Assets
$0
Total Assets
$25,000
Total Requirements
$150,000
Start-up Funding
Start-up Expenses to Fund
$150,000
Start-up Assets to Fund
$25,000
Total Funding Required
$175,000
Assets
Non-cash Assets from Start-up
$0
Cash Requirements from Start-up
$25,000
Additional Cash Raised
13. $150,000
Cash Balance on Starting Date
$175,000
Total Assets
$175,000
Liabilities and Capital
Liabilities
Current Borrowing
$0
Long-term Liabilities
$0
Other Current Liabilities (interest-free)
$0
Total Liabilities
$0
Capital
$175,000
Planned Investment
Owner
$25,000
Investor
$150,000
Additional Investment Requirement
14. $0
Total Planned Investment
$150,000
Loss at Start-up (Start-up Expenses)
($150,000)
Total Capital
$25,000
Total Funding
$175,000
Financial Indicators
Our projections assume that operations will kick off in
November, 2013 with 80 adult consumers. With these numbers,
we expect gross total revenue between December of 2013 and
March of 2014 to be 106,060. In 2014/2015, our first full year
of operation, consumer volume are projected to be 900.Our
annualized revenue will be 757,980.
Total operating costs (administrative, personnel and payroll
expenses) for 2014/2015 will show a deficit of ($37,899). This
amount does not include the start-up funding which is projected
as indicated above at $175,000. By 2015, net income will be a
15% increase from prior year which will be $871,677. As a
result of our profit margin for year ending 2015 which is
estimated to be 113,697 variance from prior year. Appendix
COOL FY 2013/14
MONTHS
Dec
Jan
Feb
22. 125
125
125
Physician Cost
5,000
5,000
5,000
15,000
Total Direct Cost
24,840
24,840
24,840
74,520
The above figures assume commencing operations with 50
enrolled consumers in October, 2011and increasing enrollment
to 70 by December, 2011.
MULTICULTURAL REVENUE 2011
MONTHS
Oct
Nov
Dec
Total
MULTICULTURAL
63. NET INCOME 2012
-23,521
-23,521
-23,521
276
276
276
276
276
276
276
276
276
-68,079
References
Daily, D., Ardinger, H., & Holmes, G. (2000). Identification
and evaluation of mental retardation. Retrieved May 3, 2011,
from http://www.aafp.org/afp/20000215/1059.html
Fletcher, R. (n. d.). Information on dual diagnosis. Retrieved
May 3, 2011, from
http://www.thenadd.org/pages/about/ddinfo.shtml
InCrisis (December 12, 2008). The Prevalence of Mental Health
and Addictive Disorders. Retrieved May 3, 2011, from
http://www.incrisis.net/Articles/PrevalenceMHProblems.htm
United States Surgeon General (1999). Mental health: A report
of the Surgeon General. Retrieved May 3, 2011, from
http://www.surgeongeneral.gov/library/mentalhealth/chapter2/se
c2_1.html
United States Surgeon General (2000). Mental health: Culture,
64. race, and ethnicity; a supplement to Mental health: A report of
the Surgeon General. Retrieved May 3, 2011, from
http://www.surgeongeneral.gov/library/mentalhealth/cre/execsu
mmary-1.html
Board of Directors
President/CEO
Clinical Director
Therapist
Addiction Clinicians
Medical Director
Psychiatrist
Psychologist
Nurse
CFO
Billing Staff
Receptionist
66. 2015Consumers Served1125
Business Plan/2
Evidence-Based Practice Project Format
Use the following format and headings when constructing your
final evidence-based practice project proposal paper for HCA
699.
1) Title page
2) Abstract (350-500 words)
a) Contains project title, project director’s name, and
affiliation.
b) Presents a complete and concise overview of all phases of the
proposed project.
3) Section A: Problem Description
4) Section B: Literature Support
5) Section C:
Solution
Description
6) Section D: Change Model
7) Section E: Implementation Plan
8) Section F: Evaluation
9) Appendices
67. a) Critical Appraisal Checklists
b) Evaluation Table
c) Conceptual Models
d) Timeline
e) Resource List
f) Proposal Instruments
g) Data Collection Tool
h) Budget
i) Optional
i) Approval Forms
ii) Handouts
iii) Evaluation Tools
HCA 620: Evidence-Based Practice Project Student Example
Table of Contents
Generating Evidence for Evidence-based Practice
Part 1: Introduction
1. The problem statement
………………………………….……………………....……….3
1. The evidence-based question
68. ………………………………………..……….……….…4
Part 2:Assemble relevant evidence & related literature
1. Locating credible
evidence………………………………………………….…...………
3
1. Appraise the
evidence……………………………………………………….……...
……4
Part 3:Implementation of the intervention
1. Planning of
change………………………………………………………………..
…....8-9
1. Clinical protocol and pilot
project………………………………………………9-14 & 23
1. Integration and Maintenance
…………………………………………………….…..14-15
1. Barriers and
strategies………………………………………………….…………
…15-18
Part 4: Conclusion
………………………………………………..………………………
…….18
Part 5:
References……………………………………………………………
………………20-22
69. Part 6: Appendices
…………………………………………………………..…………….
……23
I. Management of Mechanically Ventilated Patients: Pilot
Project ……………………23-24
II. Questions for Patient Ventilator Rounds
………………………………………………..25
III. Methodological matrix
………………………………………………………………26-28
IV. Prevention In-Service Flyer
………………………………………………………….…29
Problem Statement
The development of pneumonia caused by mechanical
ventilation is a significant problem in the intensive care units of
hospital facilities. Ventilator-associated pneumonia (VAP) is
the “most commonly reported healthcare-acquired infection” in
patients requiring mechanical ventilation support (Garcia et al.,
2009, p. 524). One of the most common reasons for an ICU
admission is related to respiratory distress or failure. VAP is
described as a form of nosocomial infection which occurs after
the first 48 hours of receiving mechanical ventilation
(Augustyn, 2007). The length of stay (LOS) for patients
70. developing VAP is higher than those never requiring mechanical
ventilation by an increase of approximately six days (Garcia et
al. 2009). In intensive care units (ICUs) across the United
States (US), ventilator-acquired pneumonia also results in
prolonged periods of actual mechanical ventilation, the excess
use of antimicrobial products, increased utilization of
healthcare resources and costs, and significant increase in
morbidity and mortality (Coffin et al., 2008). Garcia et al.
(2009) found on average, estimated costs of an additional $11,
897 to $150,841 per individual case were spent. VAP has a
significant economic impact on our society, costing hospitals
money which potentially could have been saved.
Numerous risks factors contribute to the development of
ventilator-acquired pneumonia as mechanical ventilation
presents a unique set of challenges for the patient requiring
intubation and ventilator support. Rigorous clinical studies
show oral secretions pose an increased risk for developing VAP
(Augustyn, 2007). Treatments, strategies and evidence-based
interventions have been developed to decrease the risks and
reduce the prevalence of VAP. There is evidence indicating the
use of oral chlorhexidine and the removal of oral secretions
before position changes may diminish the risks of developing
ventilator-acquired pneumonia. By reducing the levels of
bacteria in the oropharynx there would theoretically be a
decrease in the prevalence of nosocomial pneumonia (Houston
71. et al., 2002). Research demonstrates the use of 0.12%
chlorhexidine gluconate oral rinse (CHX) pre and
postoperatively reduces the incidence of VAP in patients who
are intubated greater than 24 hours. Foreground Question
In adults supported with mechanical ventilation, what is the
effect of oral chlorhexidine use and removal of oral secretions
prior to position changing on the development of ventilator-
acquired pneumonia?
Review of Evidence and Synthesis of Literature
This is a literature analysis of research reports and literature
reviews which studied the effects of removal of oral secretions
prior to position change on the occurrence of VAP. A summary
of the articles can be found in Appendix C. The studies varied
in design; from randomized to non-randomized, placebo, to
longitudinal and a pilot study. Strength for each study is noted
at Level II on the hierarchy as each one is a randomized or
nonrandomized clinical study. The research supports our
clinical question and was utilized with the development of
additions to be incorporated into the already existing ICU VAP
protocol.
The studies focused on in this review consisted of evidence
evaluating oral secretion removal and the use of chlorhexidine
gluconate oral rinse to prevent VAP. The cost effectiveness of
these interventions was found to be significant. Studies showed
oral secretions as being the medium to carry pathogens within
72. the oropharyngeal site down into the respiratory track. The
literature hypothesized removing oral secretions prior to the
position change of a patient can prevent or minimize the
movement of organisms into the respiratory tract which lead to
VAP development. Some researchers also concluded the
significance of chlorhexidine use for reducing nosocomial
infections. The combination of both interventions creates a
profound effect on reducing VAP occurrences its research
importance, which this practice change aims to strongly
support.
The review of literature consists of evidence dating from 1996
to 2008, indicating the need for continued research and close
monitoring of clinical practice changes based on the best
evidence at the moment. This problem was identified long ago
and yet still needs further evidence for best practice. Three
articles discuss removing oral secretions prior to position
changes of patients which are one of the two independent
variables of interest for this review. In one of those studies,
VAP was diagnosed in 24 of 159 patients in the control group,
but only in five of 102 patients in the study group within the
study group receiving oral suctioning prior to all position
changes (Chao, Chen, Wang, Lee, & Tsai, 2008). A similar
study showed VAP occurrence at 2.6% in the study group and
11% in the control group with probability of < 0.001 (Tsai, Lin,
Chang, 2008).
73. Studies by DeRiso et al. (1996) and Houston et al. (2002) each
sought to evaluate the efficacy of oropharyngeal
decontamination on nosocomial infections in patients
undergoing heart surgery using CHX before and after surgery.
Both DeRiso et al. and Houston et al. discovered an overall
reduced rate of VAP (52% and 69% respectively for each
study). The significance level for both studies was less than .01
(use the higher of the two) with the use of CHX with oral
suctioning of subjects for these studies.
Another related intervention assessed in a similar randomized
clinical study was the use of subglottal suctioning by Smulders
et al. (2002) and its effect on VAP incidence. This intervention
was appropriate for this review of literature; four percent of
patients who underwent continuous suctioning developed VAP
as compared to 16% in the control group. A common finding in
the studies reviewed was the savings in spite of the costs of
using CHX and equipment for oral and subglottal secretion
removal. The majority of these studies revealed a significantly
reduced duration of mechanical ventilation and LOS in the ICU.
All research studies in this literature review, with the exception
of Tsai et al.’s study, consisted of study groups homogenous in
patient samples, which suggest effective randomization. Tsai et
al.’s study has patient heterogeneity (of both medical and
surgical ICU patients) which may have confounded the results.
Also, the results of Chao et al.’s study did yield a significant
74. difference with the distribution of patients having a history of
COPD, DM, use of antacids, and surgery. These variables were
then evaluated with logistic regression for their relationship in
VAP development, and the results of the logistic regression
showed no significant impact on the direct development.
Overall the reviews are well organized, use appropriate
language, and use mostly all paraphrasing. This review
summarizes key finding of evidence for clinical practice, and
provides similar conclusions like our study regarding
interventions to implement in practice.
This literature review consisted of all but one study which were
experimental in nature and hold “a high degree of internal
validity because of the use of manipulation and randomization”
(Polit & Beck, 2008, p. 295). Tsai et al.’s study was a time-
sequenced, non-randomized quasi-experimental study most
vulnerable to threats to internal validity out of all the literature
reviewed. But the remaining study participants in the rest of
these experimental designs were all randomized after meeting
inclusion criteria. Only two studies (by Houston et al. and Tsai
et al.) may have had questionable internal validity. Houston et
al.’s study group was large but possibly too broad with subjects
intubated for too short of a period to have the intervention be
significant. This provides evidence for the need to implement
such an intervention and continue research. This may have led
to potential Type I and II errors. Tsai et al.’s weakness was the
75. limitation of a non-randomized control study and patient
heterogeneity as previously mentioned. In addition, Chao et al.
used a staff nurse of the ICU to conduct data collection; because
it is her ICU she may want “her unit” to do well with
compliance with the study, creating bias. Also, in both this and
Smulders et al.’s studies suctioning pressure was discussed.
Internal consistency was not documented and this lack of
information affects the reliability of the measurement tools.
Selection bias does not appear to be a concern in these studies,
and there appears to be no threat of history and the groups were
mainly homogenous. Overall the internal validity of the
research in this literature review is rather strong taking into
consideration these few discussed weaknesses. Regarding
external validity, the research findings in these studies can
easily be generalized to similar mechanically-ventilated ICU
adult populations. The patient populations were representative
of the typical ICU population and because of this, external
validity is strong. Steps were taken to control characteristics
which could impact the groups being compared, and any
requirements for participants were taken into consideration
when developing the sample.
The study by DeRiso et al. was double-blinded and placebo-
controlled in design techniques, and Smulders et al.’s study
reported blinding with the radiologists in regards to reading all
X-ray reports. These techniques enhanced the internal validity.
76. The studies were each performed in only one setting, but could
very easily be replicated in another ICU environment. Tsai et al.
and Chao et al.’s studies had a period during their research
which was dedicated to educating staff on the protocol to be
implemented to the experimental group. This enhanced
intervention fidelity in both studies. Also, the individual
collecting the data from Chao et al.’s study group was a trained
staff member of the ICU floor, and such actions facilitated a
strong reaction with the intervention and validated construct.
No incentives were provided to staff members for compliance
with Chao et al.’s study, but staff was aware of the fact that the
clinical setting was being monitored and data collected based
upon their performance. However, normally nurses are not
monitored closely and corrected for actions. Education for new
changes to protocols is usually brief, and like any change, will
take some time for the staff to acclimate to.
There appears to be no apparent threat to construct validity with
the discussed literature. However one could argue the
researcher’s expectancies for desired outcomes playing an
effect. For example, Tsai et al. and Chao et al.’s studies
involved the staff received a thorough education and period of
time to learn the protocol for the study’s intervention. Knowing
the researcher’s expectations, this could “become part of the
treatment construct that is being tested” (Polit and Beck, 2008,
p. 301). Researchers appropriately balanced all concerns for
77. validity in their study.
Planning a Change
After critically analyzing the evidence, the nurse develops a
plan to apply the findings to a clinical practice. Developing a
plan for change includes identifying strategies to gain
cooperation and evaluating outcomes. Once it is decided that
evidence supports a practice change, the change agent or
facilitators must develop and test the improvement. This step
requires some preliminary planning and research. Is the
innovation practical, the evidence transferable, is the
organization ready for change, are outcomes measurable and
will is it possible to implement the EBP within the organization
(Newhouse, Dearholt, Poe, Pugh & White, 2007)? If the answers
are agreeable, the innovation must be authorized through the
appropriate organizational channels. The implementation of an
evidence-based practice is considered a quality improvement
initiative and does not require the hospital Institutional Review
Board approval. The Quality Care Committee, which oversees
process improvement, protocol, and policy changes, will review
and approve this proposed implementation of evidence-based
practice, as part of the initial planning. The planning phase
includes assessing the feasibility of change, defining the
change, identifying resources, and defining the desired
outcomes (Reavy & Tavernier, 2008).
The proposed EBP innovation is to complement the policy for
78. oral care and suctioning of mechanically ventilated patients
with a 10% chlorhexidine gluconate oral rinse and increase
suctioning to every two hours prior to repositioning. These
interventions can also be increased according to the patients’
needs. The expected outcomes of the change are improved
patient care, reduced costs related to VAP infection and
increased lengths of stay, and the reduction of the incidence of
VAP in patients mechanically ventilated for more than 24 hours.
The project feasibility is very good, due to the small scale of
the intervention, the ease of implementation into protocol
already in place, it’s compatibility with the practice
environment, and it is simple to test in a small sample
(Newhouse, Dearholt, Poe, Pugh & White, 2007). Other aspects
contributing to the project’s potential for success is the
availability of ample resources including the Quality Care
Committee, Clinical Nurse Specialist, ICU Nurse Educator, Unit
Preceptors, Clinical Managers, and Infection Control Nurse.
Implementation and Evaluation of Change
Proposed Project
The authors plan to implement changes in current policy of
management of ventilated patients as a pilot project at
Scottsdale Healthcare Shea ICU. The change will be to add
chlorhexidine rinse for oral care every two hours and suctioning
of oral secretions prior to repositioning the patient. The data
will be collected on all ventilated patients during daily
79. multidisciplinary team vent rounds by the infection control
nurse. See Appendix A for pilot project with current changes in
policy. We plan to implement the change at Scottsdale
Healthcare Shea medical surgical ICU from June 1, 2010 to
April 1, 2011.
Implementation Plan
To enhance the patient outcome during hospitalization, an
evidence-based pilot project will be implemented. As mentioned
earlier, the problem of VAP pertains to all ventilated patients in
different ICUs, but it is easier to start the pilot project in one
unit and expand it to the other ICUs of the Scottsdale
Healthcare hospitals after assessing the effectiveness of the plan
and making any necessary changes after the evaluation process.
The authors propose to implement the pilot project initially in
the ICU of Scottsdale Healthcare at Shea campus. The plan will
be presented to the ICU nurse manager, supervisors, infection
control nurse, and the clinical educator of the ICU to obtain
permission and approval in order to implement the plan. The
plan will also be presented to Quality Care Committee May
2010 meeting for their permission for the change. After
obtaining permission for the plot project, evidence base
education material containing prevalence of VAP rate, its
complications, cost, recommended change with use of
chlorhexidine gluconate in oral care, and oral secretion
80. suctioning prior to position change will be presented to the staff
during ICU Unit Base Committee (UBC). Four more teaching
sessions will be provided, two in each day and night shift, so
that staff can attend a session which is more convenient to
them. All the registered nurses working in ICU will be required
to attend one of the teaching sessions. The teaching session or
in-service will be on May 20, 2010 from 8 a.m. to 9 a.m. and
from 8 p.m. to 9 p.m. These times are chosen to make it
convenient for nurses to attend the in-service before going home
at the end of their shift. Two more teaching sessions will be
provided on May 23, 2010 from 11 a.m. to 12 noon and from 10
p.m. to 11 p.m. Six brochures to notify staff of the in-service
dates and times will be prepared and placed in the restrooms,
break rooms and in hallways within the unit (Appendix D).
A power point presentation along with two poster boards
containing evidence based information about VAP prevalence
and its outcomes and changes in practice will be prepared and
presented to staff during the in-service. One poster board will
be placed in break room and the other poster will be placed in
meeting room of ICU to enhance teaching. Time for answering
any questions will be provided at the end of the teaching
session. The teaching will be conducted in an informal way, and
the research assistant will be available to re-educate and answer
questions for staff as needed. One day shift nurse and one night
shift nurse will be prepared by the nurse educator to do the
81. teaching for the rest of the ICU staff. The physicians and
respiratory therapists of ICU will also be notified of this
evidence based plan so they will be knowledgeable about this
VAP pilot project.
The resources needed for the implementation of this plan are
two poster boards, a power point, and a jump drive to store the
teaching material. Also required would be the chlorhexidine
gluconate oral rinse, which would be ordered from pharmacy for
each ventilated patient in the intervention group. The other
resources needed are the staff education time for the RNs who
are teaching the in-service and the staff who is attending the in-
service. There are twenty-three day shift RNs and twenty night
shift RNs in ICU who will need to attend these in-services, so
one hour in-service for each RN will need forty-three hours of
education time for registered nurses in addition to five hours of
teaching time for the RNs who are teaching these in-services.
Most of the cost of this project is the cost of education time for
the staff nurses. The two poster boards will cost seven dollars
each, a small jump drive for twenty dollars and the power point
is free. The cost of chlorhexidine is also negligible when
compared with the cost of VAP. This will be the money well
spent and pay for itself with shorter length of stay of ventilated
patients due to VAP prevention or reduction. This project will
save money for the hospital by improving patient outcome and
decreasing VAP rates and the hospital length of stay.
82. Having a theoretical framework enhances the worth of the study
according to Polit and Beck (2008). This plan will be guided by
the Kurt Lewin’s change theory to improve delivery of
information to staff. Lewin’s change theory involves a three
stage model of change, which are unfreezing, change, and re-
freezing (Neil, 2004). The first stage of unfreezing involves the
concept of becoming motivated to change or unfreeze from
previous practices. In ICU, the staff will be prepared for the
change by explaining them the magnitude of the problem, so
that they feel the need for the change. They will be notified
about the statistics of VAP prevalence and the magnitude of the
complications of VAP. These measures will motivate the staff
for a change in practice.
The second stage of Lewin’s change theory is implementation of
the change. This stage is the actual stage of alteration and will
be most essential in maintaining consistency with the use of
chlorhexidine in oral care and suctioning the patients prior to
position change. Support will be provided to staff during this
stage by answering their questions and addressing any concerns
they have. The registered nurses will implement the learned
techniques of using chlorhexidine in oral care and suction
patients prior to position change every two hours and as needed
for the duration of plot project from June 1, 2010 to April 1,
2011. The multidisciplinary vent round will continue to enforce
the change and collect data on ventilated patients. The
83. physicians will also be supported and welcomed for their input
in this process.
Lewin’s final stage of the change theory is the concept of re-
freezing or making the change permanent. In this last stage of
change theory, the newly learned changes become habitual for
the staff (Neil, 2004). The staff will be reinforced and
encouraged to continue to follow the recommended changes at
each month’s staff meeting and daily multidisciplinary vent
rounds for the duration of pilot project. The staff will also be
encouraged for their feedback on this project. They will also be
reinforced about this newly learned skill at the annual skills fair
and have opportunity to get their questions answered. The
future of the healthcare is moving towards pay for performance
measures and this teaching plan will lead Scottsdale Healthcare
towards delivering a better patient outcome.
Evaluation Plan
The evaluation of this teaching plan is relatively simple. The
infection control nurse keeps the data of VAP rate of all
ventilated patients. The data including VAP rate obtained by
infection control nurse from vent rounds during the pilot project
will be compared with the VAP rate of ventilated ICU patients
of this unit from the previous year. The VAP rate during pilot
project for the months of June 1, 2010 to April 1, 2011 will be
compared with the VAP rate of previous year for the months of
June 1, 1009 to April 1, 2010 to promote validity. The types of
84. patients vary by season, and by doing this we increase the
likelihood of having a similar patient population which is
representative of the months of June to April. These findings
will be discussed among the ICU manager, supervisors, clinical
educator and infection control nurse in May 2011 upon
completion of pilot project. A decision will be taken to adopt
the change or reject the change depending on the findings if
VAP rate was reduced or not.
Dissemination Plan
The staff will be will be notified of the project completion in
monthly staff meeting in May 2011. The goal of this
dissemination plan is to utilize this new research or evidence
based information to improve patient outcome. If the finding
suggests a decrease in VAP rate during pilot project, the change
will need to be implemented to other ICUs of Scottsdale
Healthcare. All the nurses at Scottsdale Healthcare ICUs will
need to be reached to ensure that everyone can benefit from this
information. Since the problem of VAP pertains to all the ICUs
of Scottsdale Healthcare hospitals this information needs to be
disseminated to the Scottsdale Healthcare Shea CVICU, and
eventually to ICUs at Osborn and Thompson Peak campuses.
With the permission from the PCC’s chair, the committee will
be presented with recommended changes. The project will be
presented in detail and the importance of the need for a change
in practice for VAP reduction will be stressed with the
85. supporting evidence. Again the goal will be to obtain
permission to expand the changes to CVICU of Scottsdale
Healthcare Shea. Two to four nurses from each floor can be
prepared to teach the rest of the staff on CVICU. In-service
time to prepare them will be arranged at a convenient time.
The power point presentation containing the teaching material
will be made available to all the hospital employees on the
Scottsdale Healthcare Shea campus’s Special Care Unit’s web
site. This will promote access to the teaching contents for the
staff. The other sources of information will be the RNs of ICU
who performed the in-service for their staff. A copy of this plan
will be made available to the staff through Scottsdale
Healthcare Library also.
To include Osborn and Thompson Peak in the teaching plan, the
Nursing Leadership Committee will be approached, where the
nursing managers from all three campuses are available. They
will also be approached the same way as mentioned above to
disseminate the pilot project recommended changes plan to the
two other campuses. The resources, the contents of the VAP
teaching plan, and the medium will be made accessible to them
as well. A dissemination plan as mentioned above will be
carried out in a similar fashion for the other two campuses also.
Integration and Maintenance of Change
Initiating the changes to the pre-existing protocol would first
involve several steps as previously mentioned. There would be a
86. decision on who would be collecting the research data. After the
Quality Care Committee approves the change, we would select a
research assistant experienced in infection control to collect
data and monitor the process during the study. This study would
also require a qualified personal to educate the staff on the
protocol changes and be available to answer any questions
which may arise. The pilot study (see Appendix A) would then
take place. Prior to the study, daily rounds are completed on
each ventilated patient to collect information for VAP. After
implementing this study, this research assistant would
accompany the ventilator rounds team and collect information
applicable to the study. This would help facilitate monitoring
the process and outcomes of the intervention. See Appendix B
for examples of major questions included during ventilator
rounds. Questions italicized would be additions made to the
rounds during the study for data collection purposes. This
information on VAP rates and patient length of stay after
implementing the new interventions would be put together and
submitted to the appropriate committees.
Integrating the new policy on the unit, staff will be much more
likely to accept and support the new process if they know what
to expect at each phase of the change. Additionally, staff
members are able to contribute ideas drawn from their varied
experience. Staff ideas often improve the process, save money,
and avoid potential obstacles (Gotsill & Natchez, 2007).
87. Implementing this change of protocol would involve the
cooperation of both the research and hospital staff.
Communication between both groups is crucial, and a key
concept of implementing a practice change. Providing updates
to the Quality Care Committee, Infection Control Team, unit
manager, and the staff throughout the study would be crucial.
Quarterly feedback to the staff alone will help visually show
their cooperation in this study and the beneficial outcomes
yielded from the implementation change.
Barriers and Strategies of Change
The work environment healthcare professionals face daily is
demanding. Nurses manage heavy workloads and high acuity
patients along with staffing shortages and cost cuts, which
reduce all available resources. This creates challenges to
implementing new policies, protocols, or evidence-based
practice (EBP). Some of the potential barriers to implementing
EBP clinical changes can be categorized as individual,
organizational, environmental, and communication based
barriers (Udod & Care, 2006). Although it appears to be an
impossible task, there are many strategies to help gain
cooperation from the individuals responsible for implementing
change. A few strategies are managerial support, clearly written
research, exposure to real-life case studies, role modeling, staff
engagement opportunities, and psychosocial support (Udod &
Care; Thompson, Bell & Prevost, 1999).Potential Barriers to
88. Implementing EBP
Healthcare professionals have reported a variety of barriers to
implementing EBP. Nurses can be skeptical, especially if they
have misperceptions, fears, or anxiety that prevents them from
having a clear vision when implementing change (Melnyk &
Fineout-Overholt, 2005). Individual barriers include a lack of
competence of nurses and managers regarding the
implementation of EBP strategies, a lack of academic skills, and
an inability to apply research to practice as evidenced by the
large research-practice gap that exists in the profession (Udod
& Care, 2006). Overwhelming workloads may also leave nurses
drained, lacking motivation, confidence, awareness, and time
(Thompson, Bell & Prevost, 1999). Melnyk and Fineout-
Overholt state that barriers to EBP implementation and
adherence are oftentimes related to individual attitudes. A lack
of confidence in the plan or its creator, an inability to visualize
a positive outcome, or doubt in one’s own skills are a few
examples (2005).
Some individual barriers can be associated with the
organization. However, nurses must overcome other
organizational barriers. Examples are administrative constraints
such as a lack of funding for skill development, opposing
managerial priorities, or a lack of support from management and
administration (Udod & Care, 2006). Other workplace barriers
are difficulty accessing journals and evidence to support EBP,
89. peer pressure to continue traditional practices, patient demands
for widely prescribed treatment, and heavy patient loads which
prevent learning and EBP implementation (Melnyk & Fineout-
Overholt, 2005).
Nursing professionals face environmental barriers, as well, in
the implementation of EBP. EBP can be affected by government
policy or may be controlled by laws and legislation. An example
is the use of medical marijuana for nausea and anorexia in
cancer patients, which is illegal in many states. Coworkers and
managers with different agendas in the workplace can be
considered an environmental barrier to change. Occasionally an
organization has such a fast moving culture of change, it leaves
nurses too overwhelmed to cope (Udod & Care, 2006).
Finally, there are communication barriers in every aspect of
life. The implementation of EBP can be affected by a lack of
appropriate collaboration and communication between every
level of provider involved including researchers, nurses,
educators, managers, and administrators (Thompson, Bell &
Prevost, 1999). Communication errors and barriers can occur in
the educational programs and training for EBP, the
interpretation of research, and in publications and presentations
(Melnyk & Fineout-Overholt, 2005). This issue can be further
complicated with the addition of multidisciplinary involvement,
which requires another level of communication to be successful.
Strategies for Successful Implementation of EBP
90. The implementation of EBP provides for safer, more cost-
effective care with patient-specific interventions. In order to
accomplish this, organizations must employ a plan to gain
cooperation from the individuals who are responsible for
implementing the EBP. Successful implementation requires
organizational change and buy-in. The most important strategy
for EBP implementation is ensuring the support of the
organization and management. This will assist in eliminating
constraints, allow for budgeting and possibly funding for
education and incentives, and provide encouragement and
persuasion as the organization forms its opinion about the EBP
implementation (Newhouse, Dearholt, Poe, Pugh & White,
2007).
Nurses and physicians cite the desire for clearly written
research reports and exposure to case studies where EBP
resulted in improved outcomes. Providing appropriate education
and tools for EBP implementation and ensuring access to
evidence will reinforce and help providers understand the
benefits (Melnyk & Fineout-Overholt, 2005). Psychosocial
support is an important strategy, which simply means nurses are
enabled and encouraged to perform the desired change. This is
accomplished with good education, clear-cut expectations,
reinforcement, acknowledgement, and rewards. Another similar
strategy is role modeling nursing practice. This is done by
demonstrating commitment and supporting the cause for
91. advancing the EBP, while performing or educating staff about
the desired change.
Staff involvement is important when implementing change.
Strategies can include encouraging nurse participation in a
journal club or other collaborative opportunity to share
evidence. Super users, trainers, champions or stakeholders,
whatever title one chooses, can be trained to coach staff and
provide collegial support and role modeling. Staff can also
share in leadership and decision-making, give their feedback
and opinions, and contribute new ideas regarding EBP
implementation through Shared Leadership, focus groups, and
surveys. This allows the organization to measure nursing staff
knowledge, attitudes, and beliefs and identify implementation
challenges (Melnyk & Fineout-Overholt, 2005).
Conclusion
The evidence in totality supports this practice change. This
implemented change would include the variables of interest
discussed previously in the literature review and pilot plan. The
benefits of such an intervention change have the potential to
support EBP and nursing practice. Contrary to the
misperceptions many nurses have about EBP, it does not take
away from the nurses’ clinical expertise. EBP integrates the
best care with research evidence, patient’s individualized needs,
preferences and circumstances (Polit & Beck, 2006). It also
allows for exceptions in clinical setting and resource
92. constraints. EBP can also be used as a problem-solving strategy
in clinical care by taking away decisions based on custom,
authority, opinion, or ritual (Polit & Beck).
93. References
American Association of Critical-Care Nurses. (2005). AACN
procedure manual for critical
care, (5th ed.). St. Louis, MO: Elsevier Saunders.
American Association of Critical-Care Nurses (rev. 1 0/07).
AACN Practice alert: Oral
care in the critically ill. Retrieved June 3,2008 from
http://www.aacn.orgIWD/PracticeIDOCS/Oral_ Care_in_the_
Critically_1I1.pdf(Augustyn B 2007 Ventilator-associated
pneumonia: Risk factors and p
(Augustyn B 2007 Ventilator-associated pneumonia: Risk
factors and prevention)Augustyn, B. (2007). Ventilator-
associated pneumonia: Risk factors and prevention. Critical
Care Nurse, 27, 32-39. Retrieved from
http://web.ebscohost.com.library.gcu.edu:2048/ehost/search?
(Chao Y C Chen Y Wang K K Lee R Tsai H 2008 Removal of
secretions prior to position change can reduce the incidence of
ventilator-associated pneumonia for adult ICU patients: A
clinical controlled study)Chao, Y. C., Chen, Y., Wang, K. K.,
Lee, R., & Tsai, H. (2008). Removal of secretions prior to
position change can reduce the incidence of ventilator-
associated pneumonia for adult ICU patients: A clinical
controlled study. Journal of Clinical Nursing, 18, 22-28.
doi:10.1111/j.1365-2702.2007.02193.x
(Coffin S E Klompas M Classen D Arias K M Podgorny K
94. Anderson D JYokoe D S 2008 Strategies to prevent ventilator-
associated pneumonia)Coffin, S. E., Klompas, M., Classen, D.,
Arias, K. M., Podgorny, K., Anderson, D. J.,...Yokoe, D. S.
(2008). Strategies to prevent ventilator-associated pneumonia.
Infection Control and Hospital Epidemiology, 29, 31-40.
doi:10.1086/591062
DeRiso, A., Ladowski, J., Dillon, T., Justice, J., & Peterson, A.
(1996). Chlorhexidine gluconate 0.12% oral rinse reduces the
incidence of total nosocomial respiratory infection and non-
prophylactic systemic antibiotic use in patients undergoing
heart surgery. CHEST, 109(6), 1556-1561.
(Garcia R Jendresky L Colbert L Bailey A Zaman M Majumder
M 2009 Reducing ventilator-associated pneumonia through
advanced oral-dental care: A 48-mont study)Garcia, R.,
Jendresky, L., Colbert, L., Bailey, A., Zaman, M., & Majumder,
M. (2009). Reducing ventilator-associated pneumonia through
advanced oral-dental care: A 48-month study. American Journal
of Critical Care, 18, 523-532. doi:10.4037/ajcc2009311
Gotsill, G., & Natchez, M. (2007). From resistance to
acceptance: How to implement change management. Training &
Development, 61(11), 24-27. Retrieved from
http://web.ebscohost.com.library.gcu.edu:2048/ehost/search
(Hsieh H Tuite P 2008 Prevention of ventilator-associated
pneumonia: What nurses can do)Houston, S., Houghland, P.,
Anderson, J., LaRocco, M., Kennedy, V., & Gentry, L. (2002).
95. Effectiveness of 0.12% chlorhexidine gluconate oral rinse in
reducing prevalence of nosocomial pneumonia in patients
undergoing heart surgery. American Journal of Critical Care,
11, 567-570.
McEwen, M., & Wills, E. M. (2007). Theoretical basis for
nursing (2nd ed.). Philadelphia, PA: Lippincott Williams &
Wilkins.
Melnyk, B., & Fineout-Overholt, E. (2005). Evidence-based
practice in nursing & healthcare: A guide to best practice.
Philadelphia, PA: Lippincott, Williams & Wilkins.
Neil, J. (2004, June 04). Unfreeze-change-refreeze or square-
blob-star model of change. Retrieved April 10, 2010, from
http://wilderdom.com/theory/UnfreezeCgangeRefreeze.html
Newhouse, R., Dearholt, S., Poe, S., Pugh, L., & White, K.
(2007, December 1). Organizational change strategies for
evidence-based practice. The Journal of Nursing
Administration, 37(12), 552-557.
(Polit D F Beck C T 2008 Nursing research: Generating and
assessing evidence for nursing practice)Polit, D. F., & Beck, C.
T. (2008). Nursing research: Generating and assessing evidence
for nursing practice (8th ed.). Philadelphia, PA: Lippincott
Williams & Willkins.
Reavy, K., & Tavernier, S. (2008, April). Nurses reclaiming
ownership of their practice: Implementation of an evidence-
based practice model and process. The Journal of Continuing
96. Education in Nursing, 39(4), 166-172.
Smulders, K., Hoeven, H., Pothoff, I. W., & Grauls, C. V.
(2002). A randomized clinical trial of intermittent subglottic
secretion drainage in patients receiving mechanical ventilation.
CHEST, 121, 858-862.
Thompson, P., Bell, P., & Prevost, S. (1999, February).
Overcoming barriers to research-based practice. MedSurg
Nursing, 8(1), 59-63.
Tsai, H. H., Lin, F. C., & Chang, S. C. (2008). Intermittent
suction of oral secretions before each positional change may
reduce ventilator-associated pneumonia: A pilot study. The
American Journal of the Medical Sciences, 336, 397-401.
doi:10.1097/MAJ.0b013e31816b8761
Udod, S., & Care, W. (2006, October). Setting the climate for
evidence-based nursing practice: What is the leader's role?
Canadian Journal of Nursing Leadership, 17(4), 64-75.
97. Appendix A
Management of Mechanically Ventilated Patients: Pilot Project
Goals/outcomes
The patient will maintain adequate breathing pattern to provide
appropriate oxygenation and acid/base balance while providing
respiratory muscle rest. The incidence for VAP will be reduced
due to EBP pilot project interventions.
Definitions
Acid/base balance = determined by pH values from arterial
blood gas
VAP = Ventilator Associated Pneumonia
RCP = respiratory care practitioner
EBP = evidence based practice
Assessment
· Assess and document breath sounds every four (4) hours and
as needed.
· Monitor and verify ventilator settings every two (2) hours and
as needed. Assure that ventilator alarm volumes are audible at
all times.
· Monitor arterial blood gases per physician order. Notify
physician as needed.
98. Interventions
A. Wash hands with antiseptic soap and water or apply alcohol-
based hand gel before and after performing interventions.
B. The patient will be assigned to a hospital bed allowing
maximum visibility at all times.
C. Utilize oral airway if patient is obstructing oral endotracheal
tube.
D. Suction as needed; document amount, color and character of
tracheal secretions. (Utilize humidified oxygen set-up to
maximize mobilization of secretions.)
E. Reposition every two hours and as needed (unless
contraindicated), suction oral
Appendix A Continued
secretions prior to position change. Elevate head of bed to at
least 30 degrees (unless contraindicated).
F. Use oral cleaning and suction system.
1. Brush teeth and tongue a minimum of once every 12 hour
shift.
2. Provide oral care every 2 hours with chlorhexidine rinse.
3. Perform oral suctioning every two hours and prior to position
change.
G. Document and report to physician significant changes in
pulmonary status and secretions through collaboration of RCP
and RN.
99. H. Culture tracheal secretions per physician's order.
I. Keep Ambu-bag mask and adapter with patient at all times for
transport and/or emergency.
J. If the patient exhibits signs/symptoms of respiratory distress
or ventilator alarm sounds and problem cannot be quickly
identified, disconnect patient from the ventilator, manually
ventilate, and call for appropriate assistance.
K. Reduce anxiety by:
1. Explaining all procedures to the patient.
2. Providing alternative methods of communication while
intubated.
3. Re-assuring the patient that extraneous alarms are normal and
do not usually indicate an emergency situation. Indicate
appropriate medical personnel are always close by.
4. Placing the "nurse call" button within patient's reach.
5. Administering sedatives/analgesics as ordered.
L. Weaning - Follow specific weaning/extubation orders per
respiratory protocol or as written by the physician.
Supportive Data
See Reference list
Appendix B
Questions for Patient Ventilator Rounds
Patient Care Question
100. Answer from Staff
Hospital day number
Number of days ventilated
Oral care Q2
Use or Chlorhexidine with oral care*
Removal of secretions prior to position changes*
Head of bed 30 degrees
Repositioning Every 2 hours
SUP prophylaxis
DVT prophylaxis
Sedation vacation
White Blood Cell Count
Temperature (max/low in 24 hours)
101. “*” indicates interventions added to the current existing
protocol
Appendix C
Methodological Matrix and Evaluation Matrix
Author
Pub
Yr
Country
Theory
Dependent
Variables
Independent
Variables
Study design
102. Sample size
Sampling
Method
How data
collected
DeRiso, A. Ladowski, J.Dillon, T. Justice, J.Peterson, A.
2002
USA
Quanti-tative
nosocomial infections
chlorhexidine gluconate oral rinse
Prospective
randomized placebo-controlled double-blind experiment
353
Randomized surgical patients undergoing heart surgery
data analyzed of patient
outcomes after interventions complete
Houston, S.
Hougland, P.
Anderson, J. LaRocco, M. Kennedy, V Gentry, L.
1996
USA
103. Quanti-tative
nosocomial pneumonia
chlorhexidine gluconate oral rinse
Prospective
Randomized case-controlled
561
Randomized surgical patients undergoing heart surgery
Observation &Self report
Appendix C
Methodological Matrix and Evaluation Matrix Continued
Author
Pub Year
Country
Theory
Dependent Variables
Independent
Variables
Study Design
104. Sample
Size
Sampling Method
How data collected
Smulders, K., Hoeven, H., Pothoff, I. W., & Grauls, C. V.
2002
Nether-
lands
None
Incidence of VAP; duration of mechanical ventilation; length of
ICU stay; length of hospital stay; and mortality
Intermittent suctioning of subglottic secretion
with 100mg
Hg for 8 sec. duration and 20 sec. interval.
A randomized
clinical Trial
N = 150
Study group= 75
Control gp= 75
Random assignment of patients into experimental or control
group, who were admitted to ICU over 13 month period and
105. were expected to receive mechanical ventilation >3 days
Observation &
Self report
Chao, Y. C.,
Chen, Y.,
Wang, K. K.,
Lee, R.,
& Tsai, H
2008
Taipei, Taiwan
Not listed in Article but assumed by reader= Germ Theory of
Louis Pasteur
Pulmonary infection causing VAP
Removal of secretions prior to position change
2-group comparison randomized study
Control group= 159
Study group= 102
Random ICU patient admission.
Patients 18 yrs of age or older.
On a ventilator for more than 24 hours.
(Those with pneumonia before intubation or within 48 hours
106. after intubation were excluded)
Observation &
Self report from staff
Appendix C
Methodological Matrix and Evaluation Matrix Continued
Author
Pub Year
Country
Theory
Dependent Variables
Independent
Variables
Study Design
Sample
Size
Sampling Method
How data collected
H-H Tsai,
F-C Lin,
S-C Chang
107. 2008
Taiwan
None
VAP occurrence and incidence
Intermittent suction of Oral Secretions before each position
change
Quasi-exp. Non-randomized
Pilot Study
Study group= 227
Control group= 237
All patients admitted to ICU who did not have:
endotracheal intubation (EI) and mechanical ventilation
(MV) more than 3 days prior to ICU admission, presence of
tracheostomy, pneumonia before ICU admission, non-ventilated,
EI & MV < 48 Hours, ICU admission less than 48 Hours.
Self-report and observation by senior staff
Appendix DVAP Prevention In- Service FlyerVAP Prevention
108. In-service for
New Interventions!Mandatory for All Nursing Staff in ICU.
Please attend one of the following:November 20, 20108 a.m. – 9
a.m. and 8 p.m. – 9 p.m.Or
November 23, 2010 11 a.m. - 12 noon and 10p.m. - 11p.m.
HCA 620 Media: Business Plan Overview
Business Plan Overview
A business plan is a formal document stating specific business
goals, the reasons why these goals are achievable, and a
detailed guide of the pathway to success. A thorough business
plan provides a comprehensive strategy and a specific time-line
for the implementation and operations of a company or non-
profit organization. A typical business plan model can also be
adapted when a company plans a large project. It is an effective
method of communicating a company’s vision, mission, and
goals to the stakeholders that will help launch and grow the
business: Suppliers, partners, customers, patients, employees
and board members. A well developed business plan also
enables companies to gain a better understanding of the
opportunities and challenges in their market and industry.
Further, a skillfully crafted business plan that contains the
elements described below will allow a company to develop
strategies that chart the route to success.
109. There are many different business plan models. It is not a “one-
size-fits-all” proposition. Business plans need to be tailored to
the nature of the business or project. The specific needs of a
particular business or project will determine which plan is best.
While there are many different models, there are many
similarities between business plans. The wording may vary, but
several components are common to virtually all of them; you
will soon become familiar with these similarities.
Here are the sections of a typical business plan with seven
sections:
1. Executive Summary
2. Company Description
3. Product or Service
4. Market Analysis Components
5. Strategy and Implementation
6. Management Team
7. Financial Analysis
110. Here are the sections of another business plan with twelve
sections:
1. Executive Summary
2. Vision and Mission Statement
3. Business Industry and Profile
4. Business Strategy
5. Company Products and Services
6. Marketing Strategy
7. Competitor Analysis
8. Financial Forecasts
9. Loan or Investment Proposal
10. Location and Layout
11. Description of Management Team
12. Plan of Operation
Descriptions of Typical Business Plan Elements:
Executive Summary
111. The executive summary is perhaps the most important segment
of any business plan. It is not an abstract of the business plan.
Rather, it is an independent document that is engaging, clear,
and logical. It must provide the audience with the key elements
of the business, the reasons for approval, and a rationale for the
project to be implemented. It needs to include sufficient detail
for someone to decide if they want to read further.
Think of it like an elevator speech: You get on the elevator with
someone you think might invest in your company and you only
have until you reach the tenth floor to convince them to talk to
you further. The executive summary is that five minutes you
need to pique someone’s interest enough to read the entire
business plan and give it a chance. Because this section is so
important, you should write it last; it is a summary of your
entire plan.
An executive summary is usually two pages in length, briefly
describing your organization, and the product or service you
intend to provide. It should be written in a positive and
forceful manner, with the intent of convincing your readers why
your service or product is needed. Many executive summaries
will contain the company’s mission and vision, along with
marketing and financial information. The management team and
implementation strategy are often included as well. Like the
business plan itself, the content of the executive summary is
112. dependent on the nature of the product or service the company
provides. Choose a format that works best for you.
Mission and Vision
As you are certain to discover in your research, virtually all
business plans contain mission and vision statements. An
organization’s mission is the purpose for the organization’s
existence. An organization’s mission statement is a succinct
and cogent explanation of precisely what the organization does.
It is the origin of the organization’s strategic decisions. An
organization’s vision is a critical, empowering concept. It
defines what business the organization is in, and paints with a
broad and sweeping stroke the overall direction of the
organization.
Many vision statements are contained in a single sentence.
Here are the vision and mission statements of Grand Canyon
University:
Vision: Grand Canyon University is the premier Christian
University educating people to lead and serve.
Mission: Grand Canyon University prepares learners to become
global citizens, critical thinkers, effective communicators, and
responsible leaders by providing an academically challenging,
values-based curriculum from the context of our Christian
113. heritage.
Business and Industry Profile
Understanding the industry and market in which you wish to
compete is essential. Is your venture feasible? Do you have a
potential competitive advantage that can be exploited? To
develop a strategic plan on growing your business, you need to
identify the market, customers, competitors, and strategic
opportunities. Essentially, you need this information to be able
to identify the competitive advantage you can offer that will
allow you to enter this market and be successful. (Scarborough,
2011).
One highly effective method of evaluating your industry and
market is the SWOT Analysis: Strengths, Weaknesses,
Opportunities, and Threats.
1) Strengths are “positive internal factors that a company can
draw on to accomplish its missions, goals, and objectives
(Scarborough, 2011). These factors include:
a) Product: Your product and features of your product that can
provide a strategic advantage.
b) Service: How can you manage your organization and sell
your product in a way that provides you with a competitive
114. advantage? What extra can you provide?
c) Pricing: How will you market your product and strategically
place it for competitive advantage?
d) Resources: Your people and the skills, experience, and
education they bring to the venture; the capital you have
available to invest and innovate.
2) Weaknesses are negative internal factors that can prevent or
inhibit a company from reaching its goals. These are the same
factors examined under Strengths, but are those aspects that
decrease your ability to gain a competitive advantage. For
example, your product could be of lower quality than your
competitors’ because you do not have adequate capital and
human resources to produce that level of quality.
3) Opportunities and Threats are external to your company.
a) What opportunities and options exist that you can take
advantage of and exploit?
b) What threats or potential pitfalls are facing your company?
To fully evaluate your strengths, weaknesses, opportunities, and
115. threats, you need to have information about yourself, your
company, the industry, the market, and the economy. Start with
your economic sector, which is the broad category of service:
Manufacturing, retail, or distribution. Next, identify the specific
industry or industries. Within the industry, consider the
following: Market size, growth rate, potential growth trends,
stage of maturity of the industry, the effect of economic
conditions on the industry, financial characteristics,
technological advances on the horizon, and regulation or
certifications related to the industry (Abrams, 2003).
Description of Service
How do you plan to set yourself apart from your competition
and develop a successful venture? Describe your product or
service. Outline specifically what you are going to do, sell, or
provide. Are there any patents, trademarks, or copyrights?
How does your product or service compare to your competitors?
What are the key features of your product or service that will
provide a benefit to your customers? If it is a product, where
will you buy it or how will you produce it? Products or services
that are technical or unusual will need to be explained in detail.
Drawings or schematics are appropriate if they enhance the
picture you want to create of your product (Abrams, 2003).
However, make sure you describe your product with sufficient
detail to entice investors, but do it without giving away
116. proprietary or sensitive information that would reduce your
competitive advantage. This is your chance to clearly explain
the product or service to be provided. In its simplest form, this
section will explain to the reader what you plan on doing. It
will contain detailed descriptions of products and or services
your company or organization will provide. This section
explains in detail where you are now, where you want to go, and
how you want to get there. It is essentially your strategic plan
for success.
Market Analysis
Regardless of the heading names in a business plan, you will
always find some type of marketing information. Make sure
you define your customers in detail. Who are your customers?
Where do they live, what do they buy, and how many potential
customers are there for your product or service? You should
include details from the following categories: Demographics,
geographic description, lifestyle and business style description,
psychographic characteristics (e.g. technologically savvy,
conservative, socially conscious etc.), purchasing patterns, and
their view on the importance of quality, price, and convenience
(Abrams, 2003).
After you have identified your customers, you need to determine
how you will reach them. What is the best form of advertising
to reach the kind of customers you have described? What is the
message you will deliver through your advertising? How much
117. will you spend? Think about using market research in your
plan.
How will you sell your product and who will sell it? Your sales
force will be the people representing you to your customers.
What kind of sales force will you have and what personal
characteristics do you want them to have? How will you train
them and compensate them?
The following list is typical of the elements of a market
analysis:
1. Market trends, size, and growth rate
2. Target market
3. Competition
4. Industry analysis
5. Market profitability
6. Sum of the revenues of participants.
7. Advertizing and promotional plans
118. Financial Analysis
Every business plan contains some type of financial data. The
exact nature of this data is dependent on the nature of the
product or service. You will need to show financial forecasts
for several years to demonstrate the potential success of your
venture. These estimates need to be realistic and show a well-
designed operational plan that takes into account all the
expenses related to purchasing or producing your product and
selling your product or service.
The business plan should include Pro Forma Financial
Statements, including an Income Statement, Cash Projection
Schedule, and Balance Sheet. Pro forma means the statements
do not follow Generally Accepted Accounting Principles
specifically, but may include the use of estimates. Pro forma
statements will only include recurring items. For example, if
you had a fire one year and a large casualty loss, you would not
include those on pro forma statements because it is not a usual
and expected expense (Kimmel, Weygandt, & Kieso, 2009).
The figures on your financial forecasts will represent decisions
you have made about factors such as product, price, location,
customers, and strategy. It is important to be realistic about
potential sales and earnings. Be conservative and consistent;
choose an appropriate accounting method for your industry and
form of business (Abrams, 2003).
119. Many business plan financial sections will include the following
information:
1. Income statement (also called a profit and loss statement)
2. Current funding
3. Net present value (NPV)
4. Balance sheet
5. Profit and loss projection
6. Key performance indicators
7. Break-even analysis
8. Balance-sheet forecast
9. Risk analysis
10. Business ratio analysis: profitability ratios, return on sales,
return on investment, and liquidity ratios
Measurement
120. Your business plan needs to spell out how you intend to
measure the performance of your program, when you will
measure, how you will measure, what tools you will use to
report, and the frequency of reporting.
A well written business plan must include some type of
measurement data. How will you measure success? There are
many ways to measure the effectiveness of any program, and
you will need to decide which metrics make the most sense.
Generally there are two types of metrics: descriptive and
predictive. Descriptive metrics tend to be ones that are fairly
general and give a good overview of a program’s performance,
whereas predictive metrics are narrower and give an indication
of how a descriptive metric will turn out.
There are many tools that you can use to report your
performance. In healthcare the two most common methods are
charts and balanced scorecards. The term chart is often
interchanged with graph. The two most common charts are
column charts and line charts. Column charts have vertical bars
while bar charts are horizontal. In either case, they are most
useful for comparing data that is for a single point of time or
for metrics where you are expressing the data as a percent of the
whole.
A second tool for reporting is a balanced scorecard. As the
121. name implies, a balanced scorecard shows metrics reflective of
more than one category. Balanced scorecards typically measure
quality, service, employee satisfaction and financial data. By
looking at more than one area, you can make your decisions
regarding the performance of a program from more than one
viewpoint. These viewpoints are often conflicting, and
therefore a balanced score card provide a more complete look at
your program. Balanced scorecards are especially valuable in
healthcare, as decisions often need to be made on more than just
financial performance and quality.
Whatever metric you choose, it needs to be easily understood.
The data needs to be comprehensible, meaningful, and relevant.
Careful consideration needs to be given to the amount of detail
presented: Give just enough information for your reader to
understand the significance of the data. Sometimes “less is
more.”
Plan of Operation
The operational plan deals specifically with the internal
operations and equipment necessary to produce a product or
provide a service. It needs to answer several questions: Where
will your business be located? What type of building is needed?
How big does it need to be? What about office and storage
space?
122. The operational plan also deals with specific equipment issues.
This section describes the types and prices of the equipment
necessary for your business to be successful. Will you purchase
or lease? Where will you obtain and store needed materials?
Outline your key suppliers, the purchasing process, and any
other relevant supply concerns.
In addition to describing your equipment needs, the operational
plan also outlines the human element. How many employees
are needed? Are they full or part-time? Are they salaried or
hourly? How much will they earn? What will their work hours
be? How will you recruit the type of people you need? This
section deals with roles, job descriptions, management
structure, and training issues. As with the other elements of the
business plan, the exact nature of the business will dictate what
information is needed and relevant.
References
Abrams, R. (2003). The successful business plan (4th ed.). Palo
Alto, CA: The Planning Shop.
Kimmel, P. D., Weygandt, J. J., & Kieso, D. E. (2009).
Accounting: Tools for business decision-making (3rd ed.).
Hoboken, NJ: John Wiley & Sons, Inc.
123. Scarborough, N. M. (2011). Essentials of entrepreneurship and
small business management (6th ed.). Boston: Prentice Hall.
U. S. Small Business Administration (SBA). (n.d.). Small
business planner. Retrieved August 24, 2010, from
http://www.sba.gov/smallbusinessplanner/index.html
HCA 620 MEDIA: Capstone Project
A major objective of HCA 620 is to prepare students for their
final capstone project that will be due at the end of their
academic program in HCA 699 Evidence-Based Research
Project. This is the culminating activity of all previous
coursework. Your capstone project is a major endeavor
requiring a considerable amount of planning, research, and
writing. If a student waits until they are actually enrolled in
HCA 699 to begin working on their capstone project, disaster is
the likely result. Therefore, students are required to demonstrate
the progress of their capstone project in HCA 620.
This is the official course description of HCA 699 Evidence-
Based Research Project:
This capstone course provides an opportunity for students to
complete the development of a comprehensive evidence-based
project, plan, or proposal that addresses a problem, issue, or
124. concern in their professional practice and can be implemented
upon completion of the program. Projects address a problem
amenable to research-based intervention; include a relevant and
comprehensive literature review; propose a solution; and
include a fully developed program, project, or business plan.
The project also contains all the necessary information to
implement the proposed solution, evaluate its outcome(s), and
disseminate the findings. Prerequisite: HCA 675.
Evidence-Based Research Project Proposal Overview
1) Throughout HCA 699 Evidence-Based Research Project you
will develop a formal, evidence-based practice proposal.
2) The proposal is the plan for an evidence-based research
project designed to address a problem, issue, or concern in the
professional work setting. Although several types of evidence
can be used to support a proposed solution, a sufficient and
compelling base of support from valid research studies is
required as the major component of that evidence. Proposals are
submitted in a format suitable for obtaining formal approval in
the work setting. Proposals will vary in length depending upon
the problem or issue addressed; they can be between 3,500 and
5,000 words. The cover sheet, abstract, references page, and
appendices are not included in the word limit.
3) Section headings and letters for each section component are
125. required. Responses are addressed in narrative form in relation
to that number. Evaluation of the proposal in all sections is
based upon the extent to which the depth of content reflects
graduate-level critical-thinking skills.
4) The Evidence-Based Research Project Proposal will contain
six formal sections:
a) Section A: Organizational Culture and Readiness Assessment
b) Section B: Problem Description
c) Section C: Literature Support
d) Section D: