Call Girls Ooty Just Call 9907093804 Top Class Call Girl Service Available
46 Electrolyte Replacement
1. Calcium, Phosphate and Magnesium Replacement
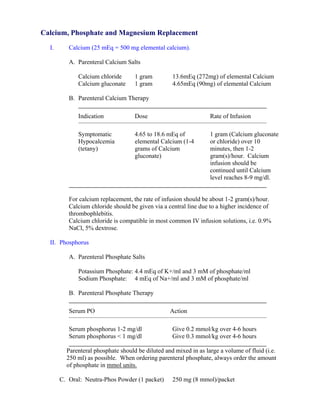
I. Calcium (25 mEq = 500 mg elemental calcium).
A. Parenteral Calcium Salts
Calcium chloride 1 gram 13.6mEq (272mg) of elemental Calcium
Calcium gluconate 1 gram 4.65mEq (90mg) of elemental Calcium
B. Parenteral Calcium Therapy
Indication Dose Rate of Infusion
Symptomatic 4.65 to 18.6 mEq of 1 gram (Calcium gluconate
Hypocalcemia elemental Calcium (1-4 or chloride) over 10
(tetany) grams of Calcium minutes, then 1-2
gluconate) gram(s)/hour. Calcium
infusion should be
continued until Calcium
level reaches 8-9 mg/dl.
For calcium replacement, the rate of infusion should be about 1-2 gram(s)/hour.
Calcium chloride should be given via a central line due to a higher incidence of
thrombophlebitis.
Calcium chloride is compatible in most common IV infusion solutions, i.e. 0.9%
NaCl, 5% dextrose.
II. Phosphorus
A. Parenteral Phosphate Salts
Potassium Phosphate: 4.4 mEq of K+/ml and 3 mM of phosphate/ml
Sodium Phosphate: 4 mEq of Na+/ml and 3 mM of phosphate/ml
B. Parenteral Phosphate Therapy
Serum PO Action
Serum phosphorus 1-2 mg/dl Give 0.2 mmol/kg over 4-6 hours
Serum phosphorus < 1 mg/dl Give 0.3 mmol/kg over 4-6 hours
Parenteral phosphate should be diluted and mixed in as large a volume of fluid (i.e.
250 ml) as possible. When ordering parenteral phosphate, always order the amount
of phosphate in mmol units.
C. Oral: Neutra-Phos Powder (1 packet) 250 mg (8 mmol)/packet
2. III. Magnesium
A. Magnesium Salts: Magnesium (elemental) 1 gram = 83.3 mEq
Magnesium sulfate 1 gram = 8.1 mEq
B. Oral Preparation: Mg Chloride 535 mg = 64 mg (5.33mEq) Mg/tablet
Mg gluconate 500 mg = 27 mg (2.25 mEq) Mg/tablet
Mg oxide 400 mg = 241.3 mg (20.1 mEq) Mg/tablet
Magnesium Citrate 1.745 gram/30 ml
C. Parenteral Magnesium Therapy
In patients with normal renal function, up to 50 mEq (6 grams) of magnesium may
be given IV over 4 to 6 hours (usually infuse 1 gram/hour), mixed in 50 to 100 ml of
0.9% NaCl or 5% dextrose.
Magnesium sulfate is incompatible with soluble phosphates and with alkali
carbonates and bicarbonates (except in dilute solutions).
3. DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center in
conjunction with the Pharmacy Department. They are intended to serve as a general statement regarding appropriate patient care
practices based upon the available medical literature at the time of development. They should not be considered to be accepted
protocol or policy, nor are intended to replace clinical judgment or dictate care of individual patients.
ADULT ELECTROLYTE REPLACEMENT PROTOCOLS
SUMMARY
Standing electrolyte replacement protocols are available for use in adult patients admitted to Orlando
Regional Healthcare hospitals. These are instituted upon direct physician order entry into Sunrise XA.
The protocols are listed below.
SPECIFIC REQUIREMENTS:
• Intravenous piggyback infusions of electrolytes must be administered with free-flow protected infusion
devices (i.e. infusion pump).
• Patients must meet the following criteria prior to initiation of the Potassium, Magnesium, or
Phosphorus protocols:
o SCr < 2 mg/dL
o Weight > 40 kg
• The electrolyte replacement protocols, Calcium chloride (Level I areas only) or Calcium gluconate (all
levels of care), Magnesium sulfate, Potassium chloride, or Potassium Phosphate, may be ordered
individually or in combination.
POTASSIUM REPLACEMENT PROTOCOL – INTRAVENOUS
• Recommended rate of infusion is 10 mEq/h
• Maximum rate of intravenous replacement is 20 mEq/h with continuous ECG monitoring (the
maximum rate may be increased to 40 mEq/h in emergency situations – see Policy #5080)
• Standard Concentrations: 10 mEq/50 mL, 10 mEq/100mL, 20 mEq/50 mL and 20 mEq/100 mL
o Maximum Concentration for Central IV administration = 20 mEq/50 mL
o Maximum Concentration for Peripheral IV administration = 10 mEq/50 mL
Current Serum Central IV Peripheral IV Administration Monitoring
Potassium Level Administration
3.6 – 3.9 mEq/L 20 mEq IV over 2 HR x 1 10 mEq IV over 1 HR x 2 No additional action
20 mEq IV over 2 HR x 1
3.4 – 3.5 mEq/L AND 10 mEq IV over 1 HR x 3 No additional action
10 mEq IV over 1 HR x 1
Recheck serum potassium
3.1 – 3.3 mEq/L 20 mEq IV over 2 HR x 2 10 mEq IV over 1 HR x 4 level 2 hours after infusion
complete
20 mEq IV over 2 HR x 2 Recheck serum potassium
2.6 – 3 mEq/L AND 10 mEq IV over 1 HR x 5 level 2 hours after infusion
10 mEq IV over 1 HR x 1 complete
Recheck serum potassium
2.3 – 2.5 mEq/L 20 mEq IV over 2 HR x 3 10 mEq IV over 1 HR x 6 level 2 hours after infusion
complete
Recheck serum potassium
Call Physician AND Call Physician AND
< 2.3 mEq/L level 2 hours after infusion
20 mEq IV over 2 HR x 3 10 mEq IV over 1 HR x 6
complete
• If both potassium and phosphorus replacement required, subtract the mEq of potassium given as potassium phosphate from
+
total amount of potassium required. (Conversion: 3 mmols KPO4 = 4.4 mEq K )
• Call pharmacy for assistance if needed.
1 Approved 05/29/01
Revised 01/14/08
4. POTASSIUM REPLACEMENT PROTOCOL – ORAL or ENTERAL (PT)
• Standard dosage forms: KCl 20mEQ tablet or KCl 10% solution (20 mEq/15 mL)
Current Serum
Total Potassium Replacement Monitoring
Potassium Level
3.7 – 3.9 mEq/L 20 mEq KCl PO/Per feeding tube x 1 dose No additional action
3.5 – 3.6 mEq/L 20 mEq KCl PO/Per feeding tube Q2H x 2 doses No additional action
3.3 – 3.4 mEq/L 20 mEq KCl PO/Per feeding tube Q2H x 3 doses Recheck serum potassium level 4 hours
after last oral dose
3.1 – 3.2 mEq/L 20 mEq KCl PO/Per feeding tube Q2H x 4 doses Recheck serum potassium level 4 hours
after last oral dose
Call Physician AND Recheck serum potassium level 4 hours
< 3.1 mEq/L
20 mEq KCl PO/Per feeding tube Q2H x 4 doses after last oral dose
MAGNESIUM REPLACEMENT PROTOCOL
• Infusions should be no faster than 1gm of magnesium sulfate every 30 minutes.
• Standard Concentrations: 1 gm/100 mL and 2 gm/50 mL
Current Serum Magnesium Level Total Magnesium Replacement Monitoring
1.5 – 2 mEq/L 2 grams Magnesium Sulfate IV over 1 HR No additional action
2 grams Magnesium Sulfate IV over 1 HR x
0.9 – 1.4 mEq/L Recheck serum magnesium level 2 hours
2 doses after infusion complete
Call Physician AND Recheck serum magnesium level 2 hours
< 0.9 mEq/L 2 grams Magnesium Sulfate IV over 1 HR x
after infusion complete
2 doses
2 Approved 05/29/01
Revised 01/14/08
5. PHOSPHORUS REPLACEMENT PROTOCOL
• Replacement must be ordered in mmol of phosphorus.
• Recommended rate = 3mmol/hr (= 4.4 mEq/h of K)
• Maximum rate = 10 mmol/hr (= 15 mEq/h of K)
• Use SODIUM phosphate for patients with serum potassium > 4.5 mEq/L and serum sodium < 145
mEq/L
• Standard Concentrations:
o Potassium Phosphate: 15 mmol/250 mL and 21 mmol/250 mL
o Sodium Phosphate: 15 mmol/250 mL, 21 mmol/250 mL, and 30 mmol/250 mL
Current Serum
Total Phosphorus Replacement Monitoring
Phosphorus Level
2 – 2.5 mg/dL 15 mmol Potassium Phosphate IV over 4 HR No additional action
Recheck serum phosphorus level 2 hours
1 – 1.9 mg/dL 21 mmol Potassium Phosphate IV over 4 HR
after infusion complete
Call Physician AND
30 mmol Potassium Phosphate IV over 4 HR Recheck serum phosphorus level 2 hours
< 1 mg/dL
(Administered as: 15 mmol Potassium after infusion complete
Phosphate IV Q2H x 2 doses)
• If both potassium and phosphorus replacement required, subtract the mEq of potassium given as potassium phosphate from
+
total amount of potassium required. (Conversion: 3 mmols KPO4 = 4.4 mEq K )
• Call pharmacy for assistance if needed.
CALCIUM REPLACEMENT PROTOCOL
• You must specify the salt form (gluconate or chloride)
• Calcium chloride:
o Reserved for Level I areas only
o Must be administered via a central line
o Maximum rate = 1 gm IV over 10 minutes
• Calcium gluconate:
o May be used in all levels of care
o Administration via a central line is preferred; however, it may be given peripherally with
adequate IV access.
o Maximum rate = 3 gm IV over 10 minutes
• Standard concentrations:
o Calcium chloride: 1 gm/50 mL, 2 gm/100 mL, 3 gm/150 mL
o Calcium gluconate: 1 gm/50 mL, 2 gm/100 mL
Total Calcium CHLORIDE
Current Ionized Total Calcium GLUCONATE
Replacement Monitoring
Calcium Level Replacement
(Level I areas only)
1 – 1.1 mmol/L 1 gram IV over 1 HR 1 gram IV over 1 HR No additional action
0.85 – 0.99 mmol/L 2 grams IV over 1 HR 2 grams IV over 1 HR Recheck serum ionized calcium
2 hours after infusion complete
< 0.85 mmol/L Call Physician AND Call Physician AND Recheck serum ionized calcium
2 grams IV over 1 HR 3 grams IV over 1 HR 2 hours after infusion complete
3 Approved 05/29/01
Revised 01/14/08
6. Advertisement
Advertisement Scaleva from Arkema Calcium Propionate oral chelation therapy
With The New Generation Cleaning Niacet: World's largest producer Fast, Effective Safe Chelation How
Solution for the Food Industry Low dust; Granular; Crystal; Do I know? Read My Story
Medmix Systems AG www.Arkema.com Powder www.ThisCureWorks.com/HeavyMetals
multi-component www.Niacet.com
mixing and application
systems for medical
use
www.medmix.ch
offer magnesium
The Internet Journal of Internal Medicine™ ISSN: 1528-8382
sulfate
manufacture
magnesium sulfate | Home | Editors | Current Issue | Archives | Instructions for Authors | Disclaimer | Share
aluminum sulfate, with others |
monensin sodium
www.jinxingchem.com
Ads by Google Potassium Phosphorus Calcium MG Creatinine Calcium Buy
Detoxamin
the safe, gentle &
proven chelation
therapy alternative Electrolyte Replacement: A Review
www.detoxamin.com
Quality Minerals Read printer friendly
Resource Bradley J.
Visit the Largest
Nutraceuticals Buyers' Phillips MD Subscribe in a reader
Guide on the
Internet! Critical Care Share with others
www.NutraceuticalsWorld.com
Medicine
calcium chloride of
china Boston
Manufacturer of Ads by Google
Calcium Chloride high Medical Center Calcium Magnesium
quality, honest service Calcium Ascorbate
www.wfxdy.com Boston Collagen Therapy
Sodium Ascorbate
University Potassium Selenocyanate
School of
Medicine
Citation: B. J. Phillips : Electrolyte Replacement: A Review . The Internet Journal of
Internal Medicine. 2004 Volume 5 Number 1
Table of Contents
Introduction
Electrolytes
I. CALCIUM
II. MAGNESIUM
A. ORAL
MAGNESIUM
7. REPLACEMENT
B. INTRAVENOUS
MAGNESIUM
REPLACE...
III. PHOSPHOROUS
A. ORAL
PHOSPHORUS
REPLACEMENT
B. INTRAVENOUS
PHOSPHOROUS
REPLA...
IV. POTASSIUM
INTRAVENOUS
POTASSIUM
ADMINISTRA...
Clinical
information
Warnings /
Precautions
Potassium Chloride
General State...
ORAL POTASSIUM
ADMINISTRATION
GU...
Abstract
In accordance with a best practice model for the delivery of care to
ICU Patients, a process of developing protocols for the standard
replacement of fluid & electrolytes should exist in most units. This is
an important step in an evolution towards a systems-based approach
in the ICU. As a baseline for these changes, we must alter the way in
which we monitor lab values.
Introduction
8. We recommend checking “routine labs” on a 4am-4pm cycle (every 12
hours) on ALL stable ICU patients. Other phlebotomy draws should
only be performed when clinically indicated; we must become more
efficient with our use and interpretation of laboratory values.
Depending on the underlying abnormality, aggressive replacement will
be expected. During the pre-rounds at 6am, house-staff begin
addressing any underlying fluid or electrolyte deficiencies. We then
review the “morning labs” as a team during the 7am rounds and
decide further treatment. Urine electrolytes should also be followed as
deemed necessary by clinical judgment.
Our goals should be:
K > 4.0
Mg > 2.0
Phos > 3.5
Ion. Ca > 4.0
Alb > 2.5
Hct > 30.
Also, it is important to ensure that ALL of our patients are receiving
their daily requirements of the electrolytes. Oral Potassium (at least 2
mEq/kg/day) should be the routine and can either be given in divided
oral doses or added to the tube feedings (continuous replacement via
tube feedings is an efficacious method of electrolyte replacement. and
we are reviewing our current policies in this regard). If a patient is on
diuretics, then we will need to increase the oral replacement. Oral
daily Mg replacement should also become standard (either with Mg-
sulfate or Mg-oxide and should range from 400mg – 1 g/day, based on
the weight of the patient). If the oral form is not well tolerated, then
we will need to shift towards IV replacement.
Our medical and surgical approaches have proven to significantly lower
9. both morbidity and mortality over the past thirty years; they are
aggressive and have set new standards for our field. Similarly, our
routine approaches should strive for the same level of care. By
successfully implementing such a system in your ICU, you can establish
a far more efficient approach in regards to fluid and electrolyte
management. We certainly do not wish to remove clinical judgment
from the system nor create a “robotic-like” atmosphere, however we
must recognize the fact that wide variations in care do exist and at
times, lead to unacceptable clinical states. By establishing these
guidelines, we hope to create a consistent baseline in order to
improve patient safety and the overall efficiency of intensive care
units.
Electrolytes
I. CALCIUM
TREATMENT OF HYPOCALCEMIA
SYMPTOMS: Tetany, muscle spasms, lethargy, seizures
NORMAL LEVELS: Total Calcium: 8.4-10.2 mg/dl (2.1-2.6 mmol/L)
Ionized Calcium: 3.8-5.3 mg/dl (0.95-1.35 mmol/L)
CORRECTION FOR LOW ALBUMIN
For every 1mg/dl of albumin below 4 mg/dl, add 0.8 mg/dl to total
calcium
= [(4 - alb) x 0.8] + calcium
1. Determine Ca x PO4 product in mg/dl before administering calcium.
If product is greater than 60 mg/dl, there is an increased risk of
10. calcium phosphate precipitation in the cornea, lung, kidney, cardiac
conduction system, and blood vessels.
2. Determine potassium, phosphorus and magnesium levels. If the
magnesium concentration is low, it should be corrected, otherwise it
will be difficult to normalize potassium and calcium.
3. Hyperkalemia and hypomagnesemia potentiate the cardiac
neuromuscular irritability produced by hypocalcemia. Hypokalemia and
hypermagnesemia protect against the effects of hypocalcemia.
4. For each 5 units of packed RBCs transfused, administer 1-2 gms (1-
2 amps) of calcium gluconate.
5. As a guideline, the total calcium will increase by 0.5 mg/dl for every
gram of calcium gluconate given intravenously.
6. Patients who develop acute hypocalcemia after parathyroidectomy,
may require up to 10 gms of calcium gluconate intravenously in 1000
ml fluid at a rate of 1 gm/hr (100 ml/hr)
A. ORAL CALCIUM REPLACEMENT
*Absorption is variable and depends on PTH, Vitamin D, and gastric
pH.
TRADE ELEMENTAL
FORMULARY AGENTS NAME CALCIUM
Calcium Carbonate 500 mg chewable tabs Tums® 200 mg
Calcium Carbonate 650 mg tablets 260 mg
Calcium Carbonate 1250 mg tablets OsCal 500® 500 mg
Calcium Carb 250 mg + Vit D 125 IU/tablet OsCal 250 +D® 100 mg
Calcium Glubionate syrup 1.8 gm/5ml NeoCalglucon® 115 mg/5ml
11. Calcium acetate (Phos Lo®) is available for phosphate binding and not
calcium replacement in patients with renal insufficiency since its
calcium absorption is poor.
USUAL DOSE: 500- 2000 mg elemental calcium a day, in divided doses
(bid-qid)
ADVERSE EFFECT: Constipation
B. INTRAVENOUS CALCIUM REPLACEMENT
Intravenous replacement should be used if severe symptomatic
hypocalcemia exists (corrected calcium is <7.7 mg/dl) or if there is a
high risk for complications secondary to hypocalcemia.
FORMULARY AGENTS Elemental Calcium__
Calcium chloride 10 % 1 gm/10 ml syringe 272 mg (13.6 mEq)
Calcium gluconate 10% 1 gm/10 ml ampule 90 mg (4.5 mEq)___
Repeat calcium levels can be drawn the next day or sooner, if
necessary.
MAXIMUM CONCENTRATIONS: Calcium gluconate: 1 gm in 50 ml D5W
or NS
Calcium chloride*: 1 gm in 100 ml D5W or NS
*Calcium chloride should not be given IM or SC because severe tissue
necrosis may occur
INFUSION RATE: Infuse over 30-60 minutes. Rapid administration may
cause bradycardia, hypotension and vasodilation. Infiltration of IV
calcium may cause severe tissue necrosis and sloughing.
12. II. MAGNESIUM
TREATMENT OF HYPOMAGNESEMIA
SYMPTOMS: Irritability, confusion, arrhythmias, weakness,
fasciculation's, nystagmus, seizures
NORMAL LEVELS: 1.7-2.7 mg/dl
A. ORAL MAGNESIUM REPLACEMENT
For Mg levels > 1.2 mg/dl AND asymptomatic, oral* therapy may be
used:
*Oral absorption is variable with 15-50 % of a dose being absorbed.
Elemental Magnesium Usual
FORMULARY AGENTS mg mEq_____ Dose_________
MgOxide 400 mg tablets 240 20 1-2 tablets daily
MgHydroxide (MOM®) 10 ml 360 30 1-2 times a day
MgHydroxide (Maalox®) 10 ml 180 15 1-2 times a day
ADVERSE EFFECTS: Diarrhea (may be reduced by dividing daily doses)
B. INTRAVENOUS MAGNESIUM REPLACEMENT
For Mg levels < 1.2 mg/L or symptomatic or patient unable to take oral
Magnesium sulfate equivalencies: 1 gm MgSO4 =100 mg Mg= 8 mEq
Mg
SYMPTOMATIC/ASYMPTOMATIC
13. WEIGHT OR Mg < 1.2 mg/dl AND Mg > 1.2 mg/dl
< 50 kg 2-3 gm Mg Sulfate 1-2 gm Mg Sulfate
>50 kg 3-4 gm Mg Sulfate 2-3 gm Mg Sulfate
Additional doses of 1-2 gms/day of Mg sulfate may be required for
several days if the patient has not previously been receiving
magnesium.
Renal insufficiency (CLcr < 20ml/min) may require lower doses of
magnesium. Caution should be used when replacing magnesium in any
patient with renal insufficiency.
MAXIMUM CONCENTRATION: 1 gm in 5 ml D5W or NS
MAXIMUM INFUSION RATE: 1 gm over 7 minutes
Magnesium sulfate may be given IM, however it can be very painful.
Doses greater than 1 gm must be given in different injection sites.
For symptomatic patients, bolus doses of IV magnesium are required.
For asymptomatic patients, adding magnesium to the patient's
maintenance IV fluids will allow for better retention of magnesium
Repeat magnesium levels can be drawn the next day or sooner, if
necessary.
III. PHOSPHOROUS
TREATMENT OF HYPOPHOSPHATEMIA
SYMPTOMS: Anorexia, bone pain, muscle weakness, respiratory failure,
CHF, hemolysis, rhabdomyolysis
NORMAL LEVELS: 2.4 - 4.5 mg/dl (0.8 - 1.5 mmol/L)
14. 1. Determine Ca x PO4 product before administering phosphorus;
If the product is greater than 60 mg/dl, there is a risk of calcium
phosphate precipitation in the cornea, lung, kidney, cardiac
conduction system, and blood vessels.
A. ORAL PHOSPHORUS REPLACEMENT
For Phosphorus > 1 mg/dl (>0.3 mmol/L), oral therapy may be used:
FORMULARY Phosphorus Sodium Potassium
AGENTS mmol /mEq
Neutra-Phos® 8 7 7 per capsule/powder packet*
Neutra-Phos K® 8 0 14 per capsule/powder packet*
Skim milk per 8 oz 4 3 5
USUAL DOSE: 1-2 powder packets* or capsules* (8-16 mmol) of
Neutra-Phos or Neutra-Phos K po/ng tid.
*Each Neutra-phos capsule/packet must be opened and diluted with
75 ml of water before administration.
8 oz skim milk (4 mmol of Phos) tid
ADVERSE EFFECT: Diarrhea (will decrease Mg absorption)
NOTE: Magnesium, calcium and aluminum containing antacids may
bind phosphorus and prevent its absorption, so should be avoided in
patients with low phosphate levels.
15. B. INTRAVENOUS PHOSPHOROUS REPLACEMENT
For Phosphorus < 1 mg/dl (< 0.3mmol/L), IV phosphorus should be
given.
FORMULARY AGENTS Phosphorus Sodium Potassium
Potassium phosphate 3 mmol/ml 0 4.4 mEq/ml
Sodium phosphate 3 mmol/ml 4 mEq/ml 0
USUAL DOSE: For acute decreases in PO4: 0.25 mmol/kg IBW*
For chronic depletion of PO4: 0.5 mmol/kg IBW*
Renal insufficiency (CLcr <20ml/min): reduce dose by 50%
As a guideline, the phosphorus level will increase by an average of 1.2
mg/dl with a dose of 0.25mmol/kg
*IBW: Men = 50 + 2.3 (inches over 5 feet)
Women = 46 + 2.3 (inches over 5 feet)
Recommended concentrations and rate of administration:
KPhos 6 mmol / 100 ml NS or D5W over 4 hours peripherally or
centrally not to exceed 15 mmol per minibag*
NaPhos 10 mmol / 100 ml NS or D5W over 4 hours peripherally or
centrally.
Maximum concentrations and rate of administration:
Use of these concentrations and rates requires continuous monitoring
and is restricted to those areas which can provide that level of care
except in emergent situations.
16. This method of administration is NOT recommended if:
total calcium is < 7.5 mg/dL or > 11 mg/dL (corrected for albumin**)
phosphorus is > 2 mg/dL OR
significant renal dysfunction (Clcr < 10 ml/min)
KPhos 15 mmol / 100 ml NS or D5W over 2 hours centrally.*
NaPhos 15 mmol / 100 ml NS or D5W over 2 hours centrally.
*Although 15mmol of KPhos provides 22 meq of potassium which
exceeds the recommended dose of potassium per minibag (20 meq),
the maximum infusion rate of 2 hours complies with current
potassium administration guidelines (i.e., 20meq/100ml NS or D5W
over minimum 1 hour centrally).
**Correction for low albumin: For every 1mg/dL of albumin below 4
mg/dL, add 0.8 mg/dL to total calcium:
Ca corrected = [(4- albumin) x 0.8] + Ca measured
Phosphorus levels should be drawn at the end of the infusion and
should always be drawn prior to any additional doses administered.
Note: Phosphorus has historically been administered over 4 to 6 hours
due to the potential risk associated with high doses and rapid
administration (i.e., hypocalcemia, hypotension, metastatic
calcification, renal failure). However, most of this data comes from
cases of hypercalcemia treated with large doses of intravenous
phosphates in which phosphorus levels were typically normal. More
aggressive electrolyte replacement is not considered as risky.
IV. POTASSIUM
17. INTRAVENOUS POTASSIUM ADMINISTRATION
Clinical information
A. Normal serum potassium value is 4.0 - 5.0 mmol/L
B. Magnesium levels should be monitored and replacement given if
necessary since potassium repletion is ineffective in the presence of
hypomagnesemia.
Warnings / Precautions
A. Rapid infusion of KCl may cause cardiac arrest.
B. Avoid extravasation. Thrombophlebitis may result and is related to
the rate, concentration and size of vein.
C. Signs and symptoms of hypokalemia (K+ < 3.5 mmol/L)
muscle weakness 5. hypotension anorexia 6. weak pulse vomiting 7.
ECG changes: flattened ST segment, T wave heart block,
dysrhythmias inversion and U wave elevation hypotension weak
pulseECG changes: flattened ST segment, T wave
D. Risk Factors for developing hypokalemia
diarrhea, vomiting amphotericin B diuretics metabolic alkalosis
insulin beta2 agonists (e.g., terbutaline)
E. Signs and symptoms of hyperkalemia (K+ > 5.0 mmol/L)
confusion 4. flaccid paralysis listlessness, irritability 5. bradycardia
paresthesias of extremities 6. peaked T-waves on ECG, dysrhythmias
flaccid paralysis bradycardia ECG changes peaked T-waves on ECG,
18. dysrhythmias
F. Risk Factors for developing hyperkalemia
renal impairmentuse of ACE Inhibitors (captopril, enalapril, lisinopril,
etc.)use of potassium sparing diuretics (spironolactone, amiloride,
etc.)use of high dose TMP/SMX for PCP in HIV infected patients
G. Patients on digoxin are more likely to develop digoxin toxicity if K+
is low.
H. If burning or stinging sensation occurs while KCl is being given via
peripheral line, the discomfort may be reduced by the following
methods:
decrease rate of infusionreduce the concentration of KCl
Potassium Chloride General Statements
I. Potassium chloride must never be administered by IV push or IM
injection.
II. All potassium chloride infusions will be supplied by the Pharmacy
Department. These infusions will be commercially prepared in
minibags, or compounded by the Pharmacy. Potassium Chloride vials
will not be stocked in any patient care areas. Any exceptions will need
to be petitioned to the P & T Committee. In pediatric or neonatal
patients, all infusions will be administered via an infusion pump and
burette, or by a syringe pump.
III. All IV maintenance infusions with KCl at a concentration greater
than 40 mEq/L must be administered via an infusion pump.
IV. Peripheral administration
19. A. In adults, the maximum concentration via peripheral line is 10
mEq/100 ml.
B. In adults, the maximum amount of KCl available in each IV minibag
is 20 mEq. In nenoates or pediatrics only two hours worth of fluid
volume will be added to the burette at anytime. Only one hour worth
of fluid should be in a syringe pump.
C. The maximum infusion rate via peripheral line is 10 mEq per hour.
In neonates and pediatrics, the maximum infusion rate via peripheral
line is 0.5 - 1 meq/kg/hour.
V. Central administration
A. In adults, the preferred concentration via central line is 20 mEq/100
ml. The maximum concentration for fluid restricted patients is 20
mEq/50 ml.
B. In adults, the maximum amount of KCl available in each IV minibag
is 20 mEq. In neonates or pediatrics only two hours worth of fluid
volume will be added to the burette at anytime. Only one hour worth
of fluid should be in a syringe pump.
C. The maximum infusion rate via central line is 20 mEq/hr. In
neonates and pediatrics, the maximum infusion rate via central line is
1 meq/kg/hour.
VI. In adults, potassium levels must be checked after a total of 60 mEq
has been administered. Potassium levels must be checked no sooner
than 60 minutes after a given IV dose. In neonates and pediatrics,
potassium levels must be checked after a total of 1 meq/kg has been
administered.
ORAL POTASSIUM ADMINISTRATION GUIDELINES
20. A. Oral potassium chloride replacement should be considered in
asymptomatic patients with serum potassium levels < 3.8 mEq/L.
B. Adult doses from 40-100 mEq/day may be required for potassium
repletion given in 2 - 4 divided doses per day. In the neonate and
pediatric patient, 1-3 meq/kg/day may be required for potassium
repletion given in 2 - 4 divided doses per day.
C. In adults, start with 20-40 mEq/day and titrate to desired level. A
40 mEq dose may be given every 2 hours for a maximum dose of 120
mEq within a 6 hour period. In the neonate, start with 0.5 - 1
meq/kg/day and titrate to desired level with the maximum dose of 3
meq/kg within a 6 hour period.
D. When oral potassium therapy is combined with parenteral
supplementation for adults, a maximum total dose (IV + PO) is 120
mEq within a 6 hour period. For the neonate, a maximum total dose
(IV + PO) is 3 meq/kg within a 6 hour period.
E. Do not use sustained release potassium products, (e.g., KDur™)
when an immediate response is desired. The potassium chloride
powder, dissolved in water, or potassium chloride solution, should be
used for a quicker response.
F. Potassium levels must be checked after each replacement dose. If
using immediate release preparations (KCl powder), a level should be
checked no sooner than 60 minutes. If using a sustained release
product, a level should be checked no sooner than 3 hours. Patients
receiving maintenance doses of oral potassium do not require levels
after each dose.
This article was last modified on Fri, 13 Feb 09 13:39:52 -0600
21. This page was generated on Mon, 18 Jan 10 15:16:16 -0600, and may
be cached.
Home | Journals | Sponsors | Books | PubMed | Editorial Help | Privacy Policy | Disclaimer | Job Opportunities | Contact
Copyright Internet Scientific Publications, LLC., 1996 to 2010.