Downloaded 3,804 times
![Common disorders diagnosed by NCS
Peripheral neuropathy
• Mononeuropathy (ex: carpal tunnel syndrome)
• Mononeuritis multiplex (ex: vasculitides, rheumatoid arthritis, lupus
erythematosus [SLE], sarcoidosis, leprosy, Lyme disease, amyloidosis)
• Polyneuropathy (ex: diabetic neuropathy,)
Myopathy
• Muscular dystrophies (ex: Facioscapulohumeral muscular dystrophy)
• Myotonia
• Congenital myopathies
• Metabolic myopathies
Radiculopathy (problem in which one or more nerves are
affected with emphasis on the nerve root; Radix = "root")
• Nerve damage from herniated discs
Diseases of neuromuscular junction
• Myasthenia gravis](https://image.slidesharecdn.com/nerveconductionstudy-120229064827-phpapp01/75/Nerve-conduction-study-4-2048.jpg)
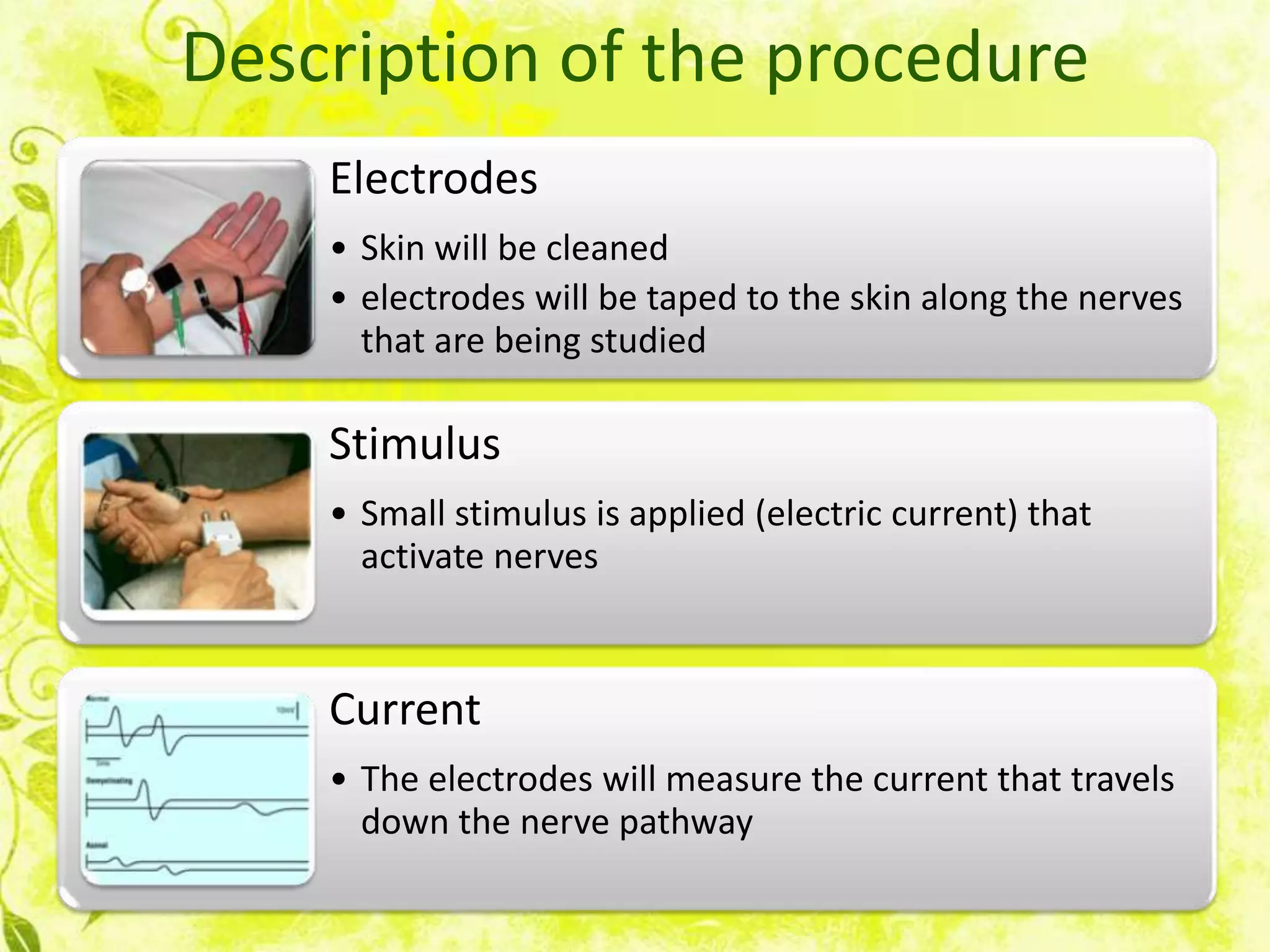
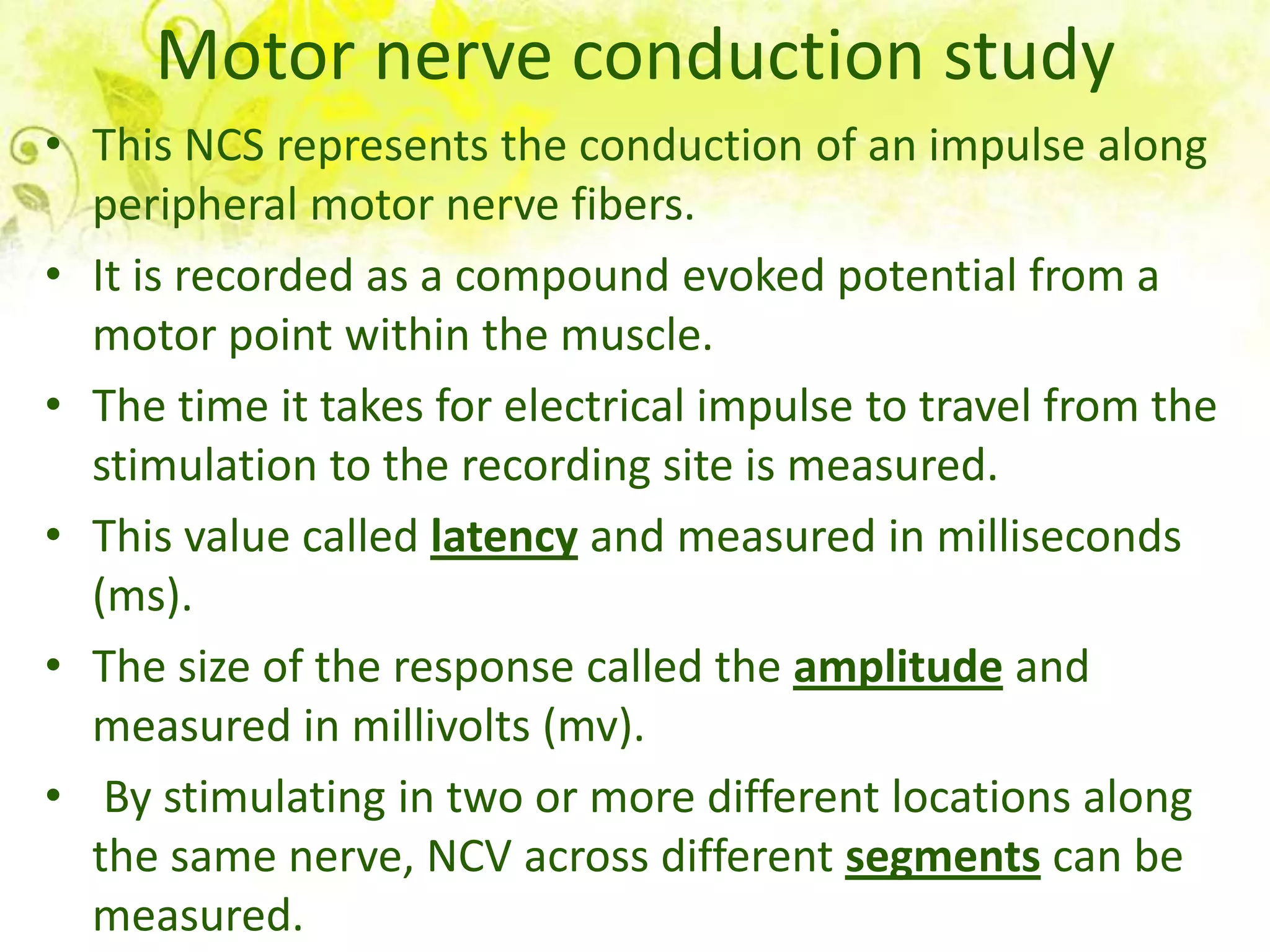

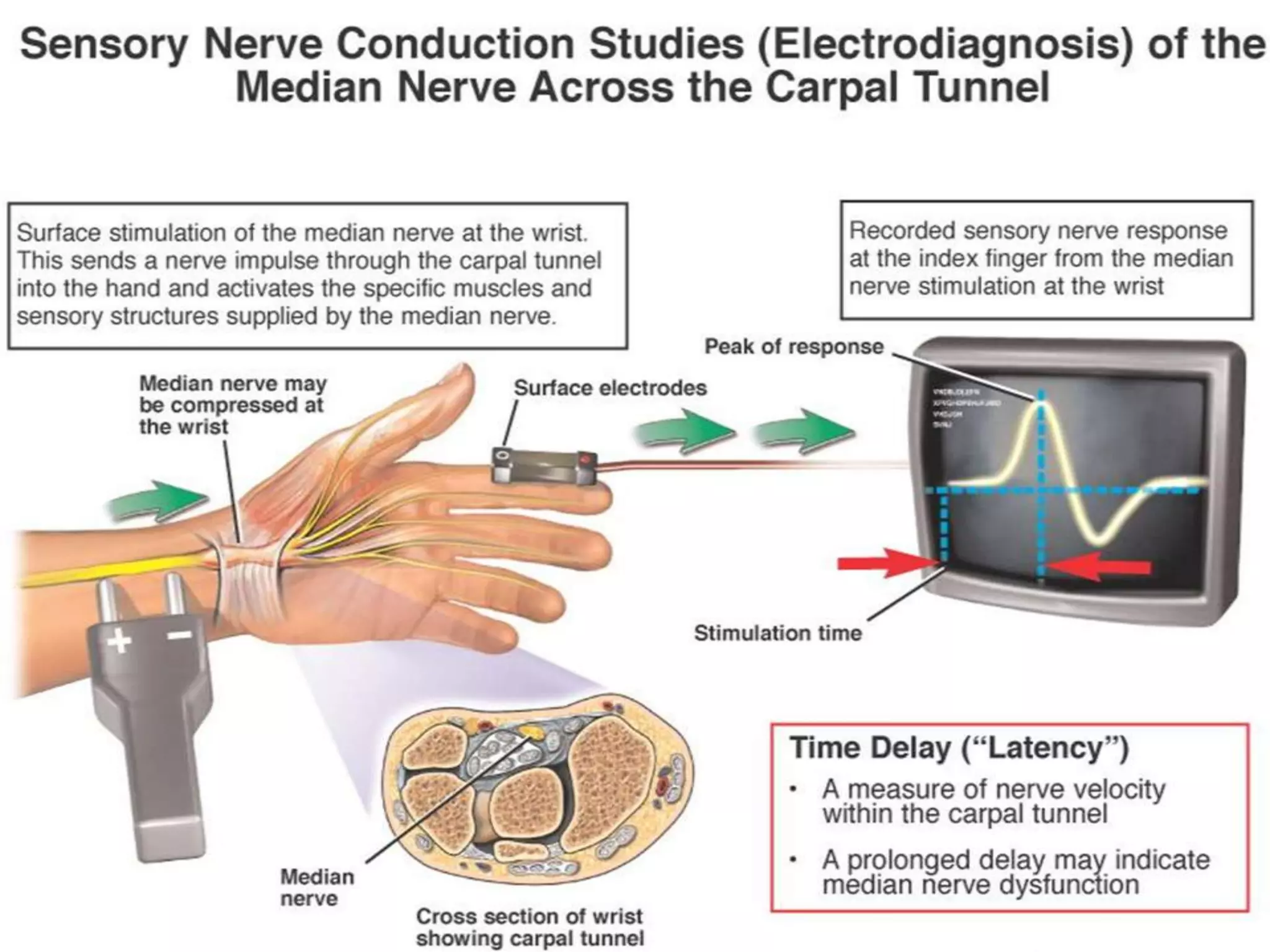
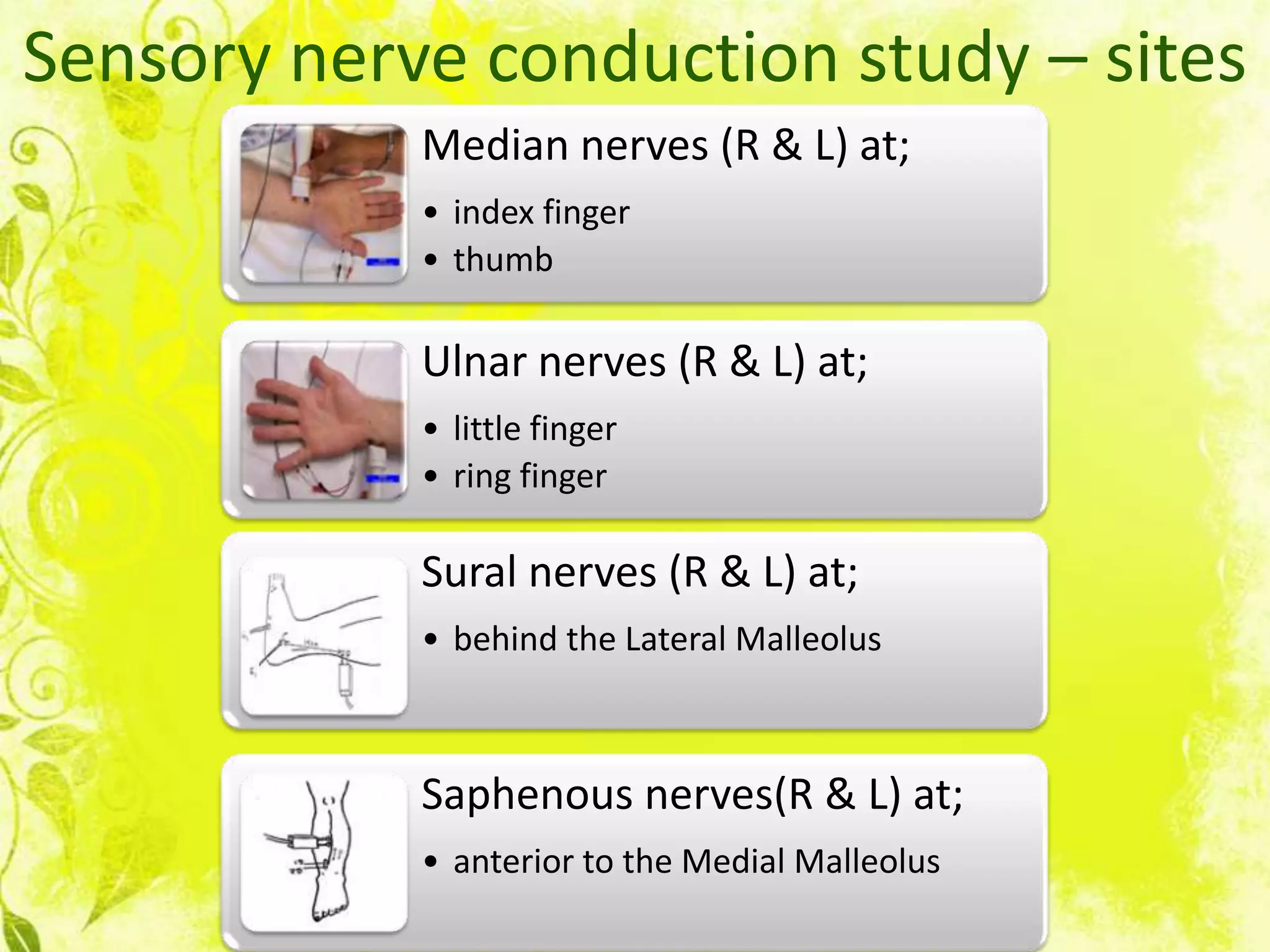



Nerve conduction studies test the function of motor and sensory nerves by measuring nerve conduction velocity. Small electrical stimuli are applied to nerves while recordings are made from muscles. Abnormalities may indicate conditions like peripheral neuropathy or radiculopathy. The test evaluates nerves like the median and ulnar nerves and can help diagnose disorders affecting the peripheral nervous system.













































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)





