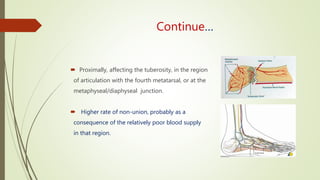
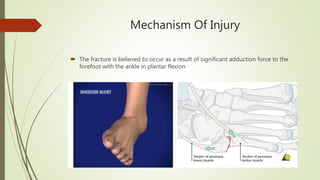
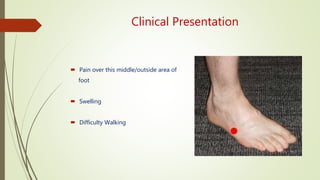
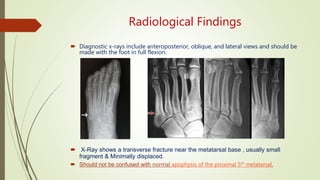
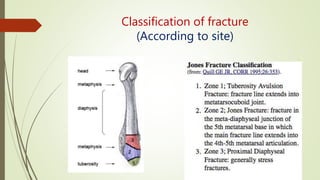
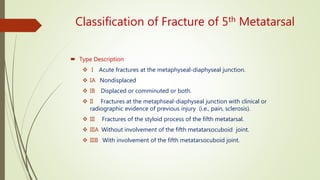
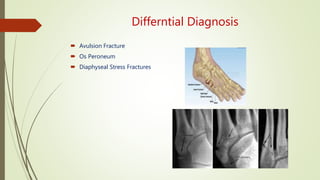
The document discusses Jones fractures, which are fractures of the fifth metatarsal bone. It defines Jones fractures, explains their anatomy and blood supply, mechanisms of injury, classification, treatment options including casting, surgery, and post-operative care. Jones fractures have a high rate of non-union due to the area's poor blood supply and are challenging to treat, especially in active patients. Surgical fixation may allow for shorter recovery times compared to casting alone.