Downloaded 610 times

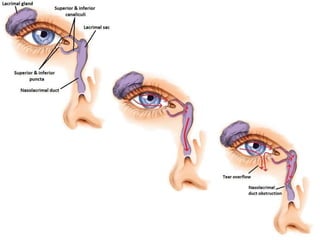
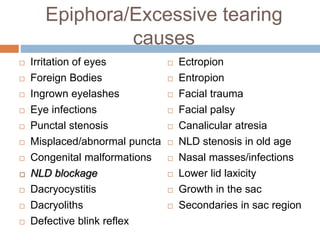
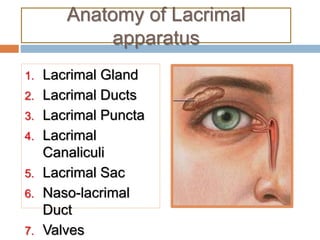
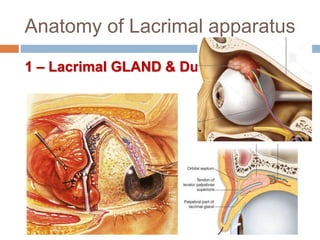

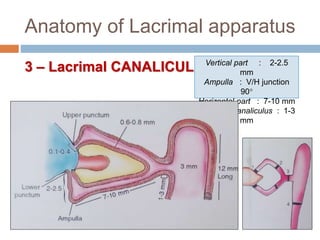
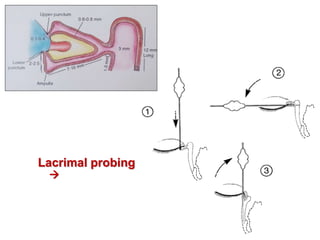

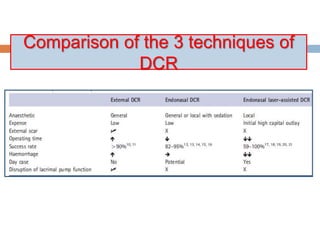
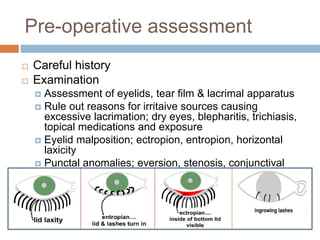




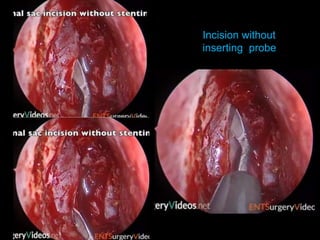
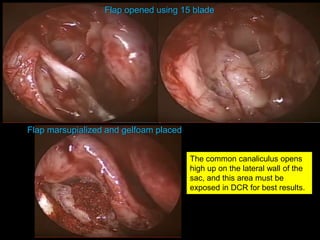
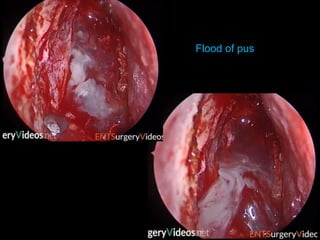

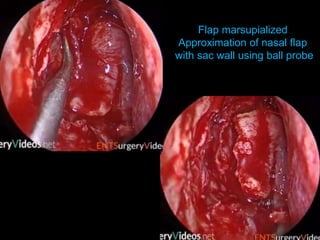
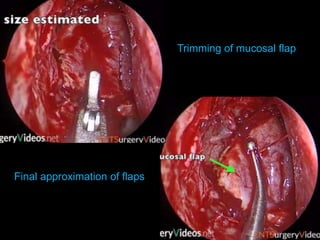
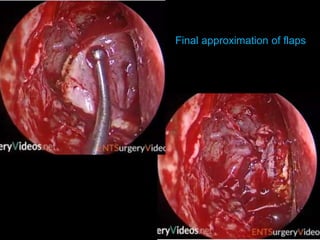
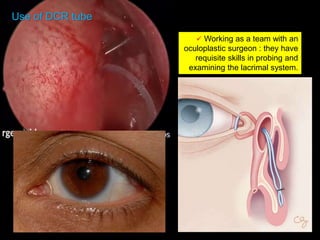


The document outlines the techniques, anatomy, and considerations related to endoscopic dacryocystorhinostomy (DCR) for treating epiphora due to nasolacrimal duct obstruction. It discusses various causes of epiphora, the advantages of endoscopic DCR over external methods, and the necessary pre-operative assessments and instruments required for the procedure. The document also highlights potential complications and causes of failure related to DCR surgeries.















































































