Downloaded 1,132 times
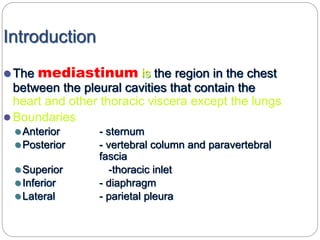
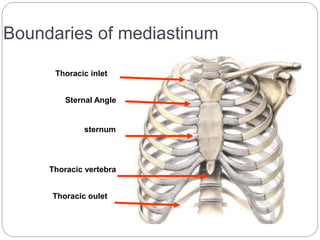
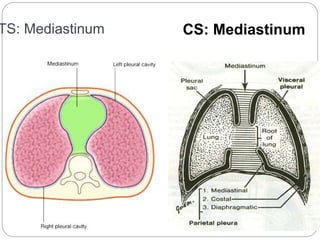
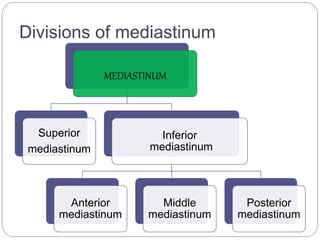
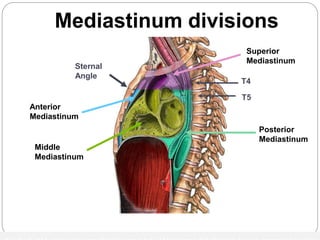
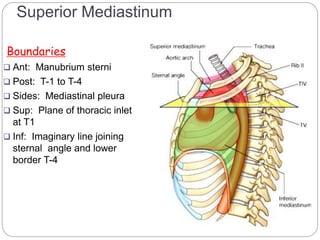

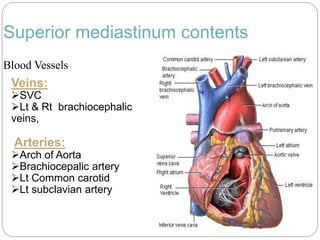
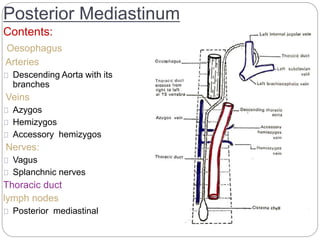
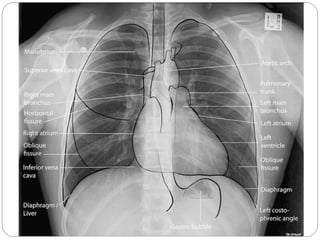
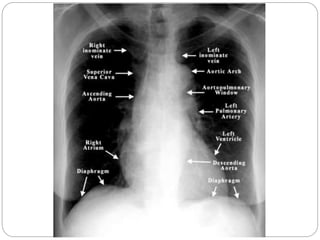
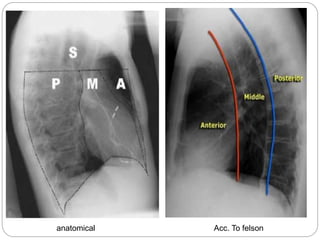
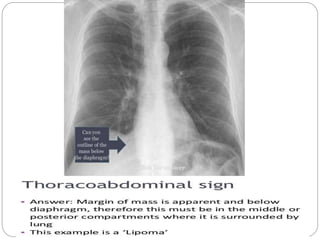
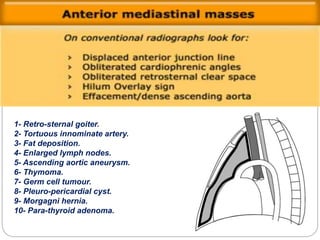
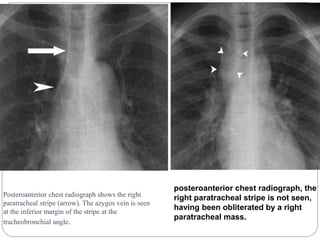
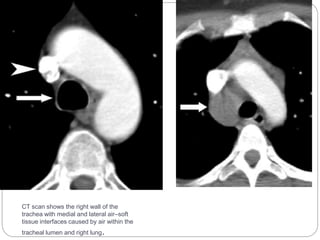
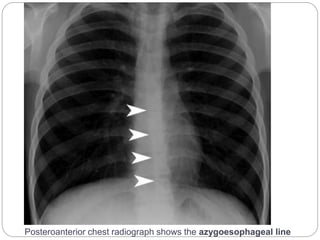




This document discusses the anatomy and radiological imaging of mediastinal masses. It begins with an introduction to the mediastinum and its boundaries. It then describes the different divisions of the mediastinum and contents of each region. Specific anatomical structures discussed include the anterior junction line, right paratracheal stripe, azygoesophageal recess, and paraspinal lines. Common masses that can occur in each mediastinal compartment are mentioned. Radiographic findings that suggest the location of a mediastinal mass are also described.



































































