Downloaded 87 times


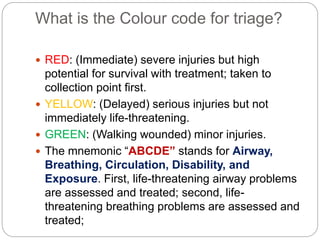
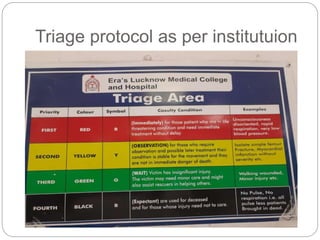
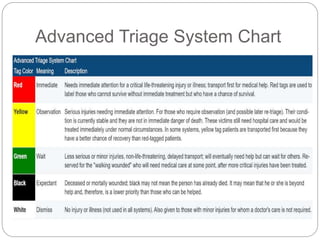
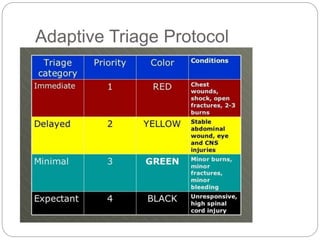
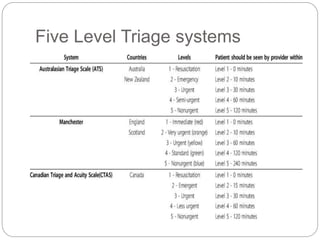
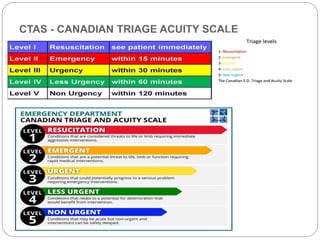
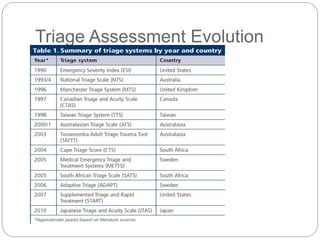

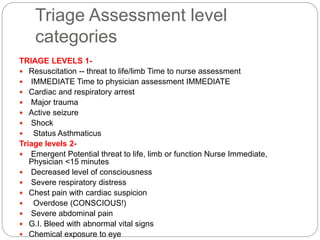
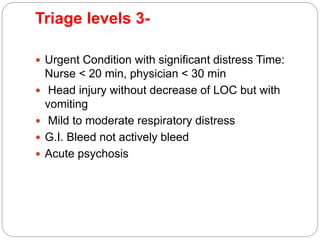
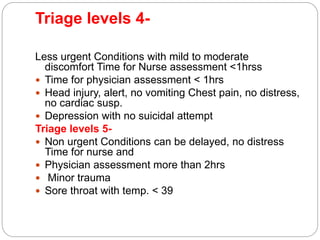
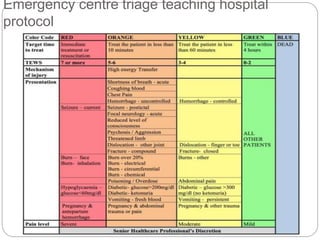
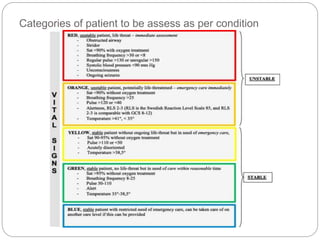


The document outlines the emergency department triage protocol for 2023, detailing the color coding system for triage, which categorizes patients based on the severity and urgency of their conditions. It discusses various types of triage, such as simple, advanced, continuous integrated, reverse triage, and explains the significance of under triage and over triage. The document further elaborates on triage levels and the assessment criteria to ensure timely medical treatment and proper resource allocation.



































































