Increased intracranial pressure
•Download as PPT, PDF•
0 likes•227 views

This document discusses increased intracranial pressure (ICP) or intracranial hypertension. It begins by describing the normal composition and pressure of the contents within the skull. Increased ICP is defined as a pressure over 20 mm Hg. Potential causes include brain injuries, tumors, hemorrhages, or obstructions in CSF flow. Signs and symptoms result from raised pressure displacing brain tissue and restricting blood flow. The document outlines medical and nursing management to reduce ICP through various interventions like medication, oxygen therapy, head positioning, and monitoring for complications.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Increased intracranial pressure
Similar to Increased intracranial pressure (20)
Recently uploaded
Recently uploaded (20)
Increased intracranial pressure
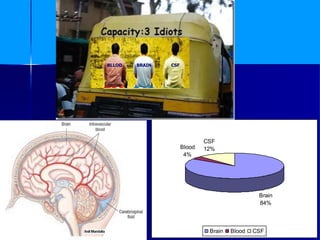
- 1. ANIL MANDALIA 1 Brain 84% Blood 4% CSF 12% Brain Blood CSF BLLOD BRAIN CSF
- 2. ANIL MANDALIA 2 INCREASED INTRACRANIAL PRESSURE (INTRACRANIAL HYPERTENSION) Our skull creates a hard casing in which our cranial contents rest and is protected from injury. The cranial contents consist of three components. Brain tissue or cells make up 84% of the cranial contents. Our cerebrospinal fluid 12% and cerebral blood volume is 4%.
- 3. ANIL MANDALIA 3 Normal ICP Intracranial pressure is the pressure exerted in the cranium by its components: Brain, blood and CSF. Normal intracranial pressure is 5-15mm of Hg.
- 4. ANIL MANDALIA 4 Definition of Increase Intracranial Pressure( intracranial hypertension) Pressure greater than 20 mm Hg is considered to represent Increase intracranial pressure or intracranial hypertension.
- 5. ANIL MANDALIA 5 Etiology and Risk Factors Brain related causes Space occupying lesion (SOL) Head injury Brain tumor Cerebral Hemorrhage Brain surgery infarction with edema Generalized brain swelling can occur in ischemic- anoxia states, acute liver failure, hypertensive encephalopathy, pseudotumor cerebri, hypercarbia.
- 6. ANIL MANDALIA 6 Increase cerebral blood flow or increase in venous pressure : Venous sinus thrombosis, Heart failure, or obstruction of superior mediastinal or jugular veins. Systemic Hypertension.
- 7. ANIL MANDALIA 7 obstruction to CSF flow and/or absorption : Hydrocephalus (blockage in ventricles or subarachnoid space at base of brain, e.g., by Arnold-Chiari malformation). Extensive meningeal disease (e.g., infectious, carcinomatous, granulomatous, or hemorrhagic). Obstruction in cerebral convexities and superior sagittal sinus (decreased absorption).
- 8. ANIL MANDALIA 8 Pathophysiology Head Injury/ Intra cranial Mass/ Brain swelling/ brain edema Increase intracranial pressure due to increase in brain tissue size or pressure.
- 9. ANIL MANDALIA 9 Displacement of CSF in to the spinal canal ( Evident by altered level of consciousness ) Further increasing in Intracranial pressure.
- 10. ANIL MANDALIA 10 Decrease cerebral blood flow through vasoconstriction of cerebral blood vessels. ( Evident by changes in EEG, altered cerebral metabolism, cerebral acidosis, brain hypoxia and brain tissue ischemia)
- 11. ANIL MANDALIA 11 Further increasing in Intracranial pressure. Herniation of the brain tissue. ( Evident by vasomotor, respiratory and cardiovascular center actions)
- 13. ANIL MANDALIA 13 Clinical Manifestations : 1. Altered level of consiousness. 2. Changes in speech. 3. Cltered pupillary reactivity. 4. Changes motor and sensory activities. 5. Headache. 6. Vomiting with no or little nausea.
- 14. ANIL MANDALIA 14 Clinical Manifestations : 7. Blured or double vision 8. Papiiledema 9. Bradycardia 10.Cheyne-strokes respiration 11.Hyperthermia 12.Brain Death
- 15. ANIL MANDALIA 15 Diagnsotic Study : X- ray Skull. C.T. Scan of brain. MRI. Transcranial Doppler. EEG. Invasive ICP monitoring.
- 16. ANIL MANDALIA 16 Management of Increase intracranial pressure : ( A) Medical Management : The main goal of medical management are to maintain cerebral oxygenation, to decrease ICP, to maintain optimal neurological function, and to ready the patient for rehabilitation.
- 17. ANIL MANDALIA 17 Maintain cerebral Oxygenation : – Oxygen inhalation to keep the PaO2 between 90-100 mm of Hg. – Endotrachial intubation. – Steroid to reduce cerebral edema.
- 18. ANIL MANDALIA 18 Decrease Intracranial pressure : – Osmotic diuretics. – Hyperventilation. – Slight head elevation. – Drain CSF
- 19. ANIL MANDALIA 19 Maintain cerebral perfusion : – Limit intra vascular fluid. – Vasoactive medication. – Barbiturates.
- 20. ANIL MANDALIA 20 Reducing fever : – Antipyretic medication.
- 21. ANIL MANDALIA 21 B. Nursing Management : Assessment – LOC – Lethargy and change in LOC first signs; restlessness – Glasgow Coma Scale – Vital signs – Late sign – Headache
- 22. ANIL MANDALIA 22 – Pupillary changes – Check pupil reaction, size, conjugate (paired; working together) . – Vomiting. – Evaluation of motor and sensory functions. – Monitoring of ICP
- 23. ANIL MANDALIA 23 Ineffective airway clearance related to diminished protective reflexes (Cough, gag) Nursing Intervention: Maintaining a patent airway. – Frequent suction. (with caution) – 100% oxygen given before and after suctioning. – Prevent suctioning more than 15 sec. – Discourage coughing. – Auscultate lung field.. – Elevate head of the bed.
- 24. ANIL MANDALIA 24 Evaluation : Evident by patent airway, breath sound clear, breath regularly, attain oxygen saturation, no secretions.
- 25. ANIL MANDALIA 25 Ineffective breathing pattern related to neurological dysfunctions. Nursing Intervention : Achieving an adequate breathing pattern. – Monitored frequently for respiratory irregularity. – Monitored PaO2 and PaCO2.
- 26. ANIL MANDALIA 26 Evaluation : Evident by regular breathing, maintain oxygen saturation.
- 27. ANIL MANDALIA 27 Ineffective cerebral perfusion related to effect of ICP. Nursing Intervention : Optimizing cerebral tissue perfusion – Elevate Head end 30 degrees with head in neutral position. – Cervical collar if needed to keep head neutral. – Avoid extreme hip flexion. – Avoid Valsalva maneuvers – ask client to exhale when being moved or turned – Avoid isometric exercises that increase SBP. – Preoxygenate and hyperventilate prior to suctioning. – Space nursing interventions. – Avoid emotional distress and frequent arousal from sleep. – Note abdominal distension.
- 28. ANIL MANDALIA 28 Evaluation : Evident by Oriented to time, place and person, follow verbal commands, improve glasgow coma scale score.
- 29. ANIL MANDALIA 29 Deficient fluid volume related to fluid restriction. Nursing Intervention : Maintain Negative fluid balance. – Monitor skin turgor, mucous membranes, serum and urine osmolality – Monitor IVF carefully. – Observe for CHF and pulmonary edema. – Good oral hygiene, monitor I&O.
- 30. ANIL MANDALIA 30 Evaluation : Evident by Optimal urine output, demonstrate serum and urine osmolality value within acceptable range.
- 31. ANIL MANDALIA 31 Risk for infection related to ICP monitoring system. Nursing Intervention : Preventing infection. – Change sterile dressing aseptically. – Aseptic technique must be adapted when managing system and changing the ventricular drainage bag. – Check the drainage for cloudiness and blood. – Watch for sign of infection viz fever, chills, neck rigidity etc. – Administered prescribed antibiotics.
- 32. ANIL MANDALIA 32 Evaluation : Evident by No fever, No signs of infection at catheter site and no purulent discharge from intracranial monitoring devices.
- 33. ANIL MANDALIA 33 Complications : Herniation of brain. Diabetes insipidus. Death.