
Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (17)
Similar to K-Endodontic scope-lec-1
Similar to K-Endodontic scope-lec-1 (20)
More from Yahya Almoussawy
More from Yahya Almoussawy (20)
Recently uploaded
Recently uploaded (20)
K-Endodontic scope-lec-1
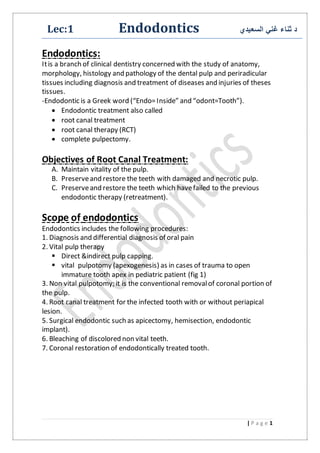
- 1. السعيدي غني ثناء دEndodonticsLec:1 1| P a g e Endodontics: Itis a branch of clinical dentistry concerned with the study of anatomy, morphology, histology and pathology of the dental pulp and periradicular tissues including diagnosis and treatment of diseases and injuries of theses tissues. -Endodontic is a Greek word (“Endo=Inside” and “odont=Tooth”). Endodontic treatment also called root canal treatment root canal therapy (RCT) complete pulpectomy. Objectives of Root Canal Treatment: A. Maintain vitality of the pulp. B. Preserveand restore the teeth with damaged and necrotic pulp. C. Preserveand restore the teeth which havefailed to the previous endodontic therapy (retreatment). Scope of endodontics Endodontics includes the following procedures: 1. Diagnosis and differential diagnosis of oral pain 2. Vital pulp therapy Direct &indirect pulp capping. vital pulpotomy (apexogenesis) as in cases of trauma to open immature tooth apex in pediatric patient (fig 1) 3. Non vital pulpotomy; it is the conventional removalof coronal portion of the pulp. 4. Root canal treatment for the infected tooth with or without periapical lesion. 5. Surgical endodontic such as apicectomy, hemisection, endodontic implant). 6. Bleaching of discolored non vital teeth. 7. Coronal restoration of endodontically treated tooth.
- 2. 2 A B C (fig 1) apexogenesis, at the time of trauma the apex was not completely formed flare up after 2 years as shown in (C) completely closed. Basic Phases of Therapy 1. The diagnostic phase, in which the diseaseto be treated is determined and the treatment plan developed. 2. The preparatory phase, when the contents of the pulp are removed and the canal prepared for the filling material. 3. Filling or obliterationof the canal to gain a hermetic seal with an inert material as closeas possibleto the cemento-dentinal junction. Indication of endodontic treatment: Unless there is a real cause to contraindicate R.C.T, All teeth with pulpal or periapical pathology are indicated for endodontic treatment which can be divided into: 1. Teeth with vital pulp. a) Acute pulpitis. b) traumatized tooth with pulp exposure. 2. Teeth with non vital pulp. a) Necrotic tooth with apical pathosis. b) Necrotic tooth without apical pathosis. 3. In some cases elective endodontic treatment is the treatment of choice,such as:
- 3. 3 1. post space: vital tooth with un sufficienttooth structure& intrapulpal extension of the final restoration (post) is needed to increasethe retention. 2. Overdenture: decoronated teeth retained in the arch to preserve alveolar bone must be root-treated. 3. Teeth with doubtful pulps: R.C.T. must be considered to the teeth with questionable state of the pulp such as direct pulp capping or non vital tooth particularly if it is to be a bridge abutment. Contraindication of endodontic treatment 1. Non restorabletooth: the tooth that cannot be restored by final crown restoration because no sound tooth structure onto which the finishing line can be placed . 2. Insufficient periodontal support: checking the mobility of the tooth must be done at the diagnostic phase . 3. Non-strategic tooth: extraction should be considered rather than endodontic treatment for unopposed and non-functionalteeth. 4. Root fractures: both vertical &horizontal fracture of the root are contraindicated unless the horizontal fracture at the level of the apical third (apicectomy can be the solution).
- 4. 4 5. Massive internal or external root resorption: both types of resorption may eventually lead to pathological fracture of the tooth. 6. Bizarre anatomy: severely curved roots, dilacerated teeth. 7. Poor oral hygiene. 8. Inadequateaccess: difficulty to reach the infected tooth due to restricted mouth opening. A simple guide to measuremouth opening is possibleto place two fingers between the mandibular and maxillary incisor teeth. Note: maxim opening of the mouth is about= 50mm, less than 35mm consider as restricted. Taking history &Clinical examination Chief Complaint The clinician must pay close attention to the actual expressed complaint fromthe patient own word. (pain, swelling, sinus or fistula, tenderness on chewing or justdiscoloration).
- 5. 5 Medical History Special dental management is needed for medically compromised patient 1. Shortvisit emergency treatment for critical cases such as pulpotomy or pulp extirpation for the patient with un stable angina, myocardial infarction, prosthetic heart valvewith prophylactic AB regimen at 1 hour before starting the dental work to decrease the chance of bacteremia & infective endocarditis: amoxicillin :1g as a single dose. clindamycin: 600mg as a single dose. (if the pt.allergic to pencillen) 2. Patient takes medication such as anticoagulant therapy, thyroid medication, and corticosteroid. • Consultation with physician. • Plain anesthesia is advisable. 5. Medical conditions can have clinical presentations that mimic oral pathologic lesions For example; tuberculosis involvement of the cervical and submandibular lymph nodes can lead to a misdiagnosis of lymph node Enlargement secondary to an odontogenic infection.
- 6. 6 Extra-oral examination: The patient’s face and neck are examined and any swelling, tender areas, lymphadenopathy, or extra-oralsinuses noted. Intra-oral examination: An assessmentof the patient’s general dental state is made: 1) General periodontal condition. 2) Presenceof softor hard swellings. 3) Discolored tooh . 4) Tooth wear and facets. 5) Intraoralsinus tracts: occasionally a chronic endodontic infection will drain through an intraoral communication to the gingival surface known as a sinus tract. This pathway, which is some time lined by epithelium, extends directly from the sourceof infection to a surface opening, on the attached gingival surface. Diagnostic tests: 1.Palpation: The tissues overlying the apices of any suspectteeth are palpated to locate tender areas. The site and size of any soft or hard swellings are noted and examined for fluctuation and crepitus.
- 7. 7 2.Percussion: Gentle tapping by dental mirror both laterally and apically on a tooth is sufficient to elicit any tenderness. It is not necessary to strike the tooth with a mirror handle aggressively, as this invites a false positivereaction from the patient. 3.Mobility: The back ends of two mirror handles should be used, one on the buccal aspect and one on the lingual aspect of the tooth 4.Radiography: In all endodontic cases, a good intra-oral parallel radiograph of the root and periapical region is mandatory. Radiography is the most reliable of all the diagnostic tests and provides the mostvaluable information. 5.Pulp testing: The electric pulp tester is an instrument which uses gradations of electric currentto excite a responsefrom the nervous tissue within the pulp. Pulp testers should only be used to assess vitalor non vital pulps, they do
- 8. 8 not to judge the degree of pulpal disease or to quantify disease. 6.Thermal pulp testing: This involves applying either heat or cold to a tooth, but neither test is particularly reliable and may produce either false positive or false negative results. A.Heat: There are severaldifferent methods of applying heat to a tooth. The tip of a gutta-percha stick may be heated in a flame and applied t a tooth. B. Cold: An ethyl chloride spray on a pledged of cotton woolor an ice stick may be applied to the suspecttooth. Icestick is made by filling the plastic covers froma hypodermalneedle with water and placing in a refrigerator. 7. Selective anesthetic: The diagnosis of the tooth with diffused pain may be challenging because of referred pain to the adjacent or opposing teeth, the patient may not even be able to specify whether the symptoms areemanating from the maxillary or mandibular arch. In these instances, the clinician should firstselectively anesthetize the maxillary arch using a periodontal ligament (intraligamentary) injection. The injection is administered to the most posterior tooth in the quadrant of the arch that may be suspected in an anterior direction, one tooth at a time, until the pain is eliminated.
- 9. 9 If the pain is not eliminated after an appropriate period of time, then the clinician should similarly repeat this technique on the mandibular teeth below. Itshould be understood that periodontal ligament injections may anesthetize an adjacent tooth and thus are more usefulfor identifying the arch rather than the specific tooth. 8. Cavity test (drilling test): When other tests have given an indeterminate result, a test cavity may be cut in a tooth which is believed to be pulpless. In the author’s opinion, this test can be unreliable as the patient may give a positive response although the pulp is necrotic. This is because nerve tissue can continue to conduct impulses for some time in the absence of a blood supply. 9. Wooden stick: If a patient complains of pain on chewing and there is no evidence of periapical inflammation, an incomplete fractureof the tooth may be suspected. Biting on a wood stick or rubber stick in these cases can elicit pain, usually on release of biting pressure.