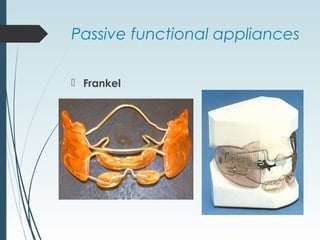
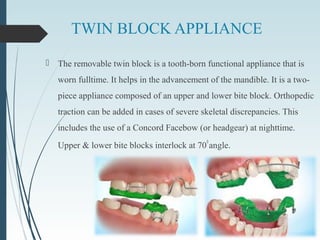
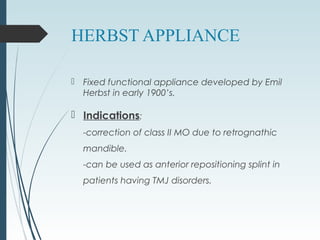
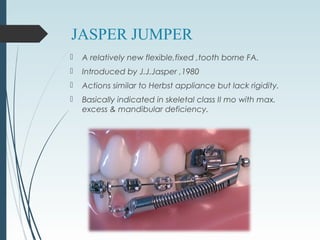
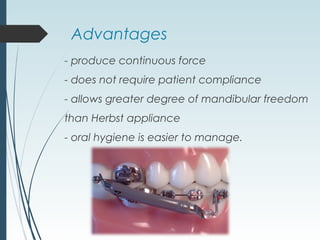
Functional appliances utilize the natural forces of the orofacial musculature to produce skeletal and dental changes. They are based on Moss's functional matrix theory which proposes that muscles and glands influence bone growth. Functional appliances can be active or passive and produce orthopedic, dentoalveolar, and muscular changes through forces of compression, elimination of restrictive influences, and mandibular repositioning. Common functional appliances discussed in the document include Bionators, Twin-Blocks, Herbst, Frankel Regulator, and Jasper Jumper. They vary in their mode of action, indications, advantages, and disadvantages.