
Recommended
More Related Content
What's hot
What's hot (20)
Similar to The congenital and acquired diseases of spine #2
Similar to The congenital and acquired diseases of spine #2 (20)
Recently uploaded
Recently uploaded (20)
The congenital and acquired diseases of spine #2
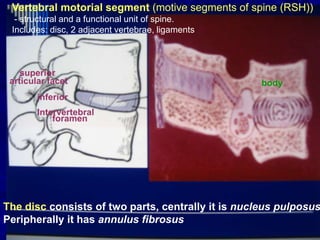
- 1. The disc consists of two parts, centrally it is nucleus pulposus Peripherally it has annulus fibrosus Vertebral motorial segment (motive segments of spine (RSH)) - structural and a functional unit of spine. Includes: disc, 2 adjacent vertebrae, ligaments foramen bodyarticular facet inferior superior Intervertebral
- 2. Remember About disc • It gives spine the mobility. • It acts as shock absorber. • It is fibrocartilaginous. • It increases the height of the spine by 25 per cent. • Centrally it has a nucleus pulposus and peripheralfy annulus fibrosus. • It is avascular. • Annulus fibres are weak posteriorly, hence posterolateral disc prolapse is more common.
- 3. Osteochondrosis – this degenerative-dystrophic disease of spine with the primary defeat of intervertebral disk, with various structural-functional violations.
- 4. AETIOLOGY OF DISC HERNIATION Risk factors •Jobs requiring heavy and repetitive weight- lifting •Obesity • Monotonous work, working overtime, • Improper postural habits etc.. In genesis of osteochondrosis of spine forming of «vicious circle» of dystrophic and degenerative changes at a different level of organization of the system of motive segments of spine (RSH) is a determinative: organ, tissue, cellular and molecular. Degenerative changes make the disc susceptible to trauma.
- 5. 1 Stages - internal disc displacements of nucleus
- 6. 2 Stages - Disc bulging or protrusion (protrusion of intervertebral disk) Central disc protrusion Intermediate protrusion Lateral protrusion
- 7. 3 Stages - disk herniation
- 8. MRI study of lumbar spine showing L4 and L3, disc prolapse, L4disk herniation
- 9. Discography and Myelography study of the lumbar spine spinal stenosis disc herniation
- 10. Discogenic instability Discarthrogenic instability Vertebral motorial segment (motive segments of spine )
- 11. Discarthroosteogenic instability facet joints degenerate and allow the forward slip Lytic fatigue fracture of the pars. This due to stress fracture
- 12. instability - Functional Radiography (flexion and extension)
- 13. Conservative therapy Osteochondrosis •Absolute bed rest is the best treatment for low backache • non-steroidal antiinflammatory drugs (NSAIDs) • muscle relaxants • traction • Flexion or extension exercises •Back braces or belts are recommended in acute stages. •Epidural steroids is a symptomatic method of treatment •Manuel therapy (subacute and chronic cases) •Chemonucleolysis ( Limited only to lumbar spine, drug used is chymopapain)
- 14. How traction helps It relieves muscle spasm It may distract the facet joints It may distract the disc space Absolute indications for surgery - Failed conservative management (6 week) . Principles of surgery is to see that the pressure on the nerve root is relieved by removing the prolapsed disc.
- 20. Чрескожная нуклеотомия со стабилизирующим эффектом B-Twin (Disc-O-Tech)
- 21. Дискектомия + задний спондилодез мет. пластинами, фасетектомия, костная пластина Open or microscopic lumbar discectomy
- 23. The amount of slippage is graded 1-4 Upper vertebral displacement over the tower vertebral body. Meyerding's classification of spondylolisthesis. G1 25 % G 2 25-50 % G3 50-70% G4 > 75% forward displacement
- 24. Clinical signs: 1.Pain in the back, buttock or thigh 2.Deformity • Palpable step at L5-S1 (at the upper angle of the sacrum). • Increased lumbar lordosis. • Torso is short • A transverse furrow encircles the body between the coastal margins and the iliac crest. • Sacrum is more vertical • Buttocks fiat and hamstring tightness • L5 spinous process prominently felt 3. Neurology • L5, or S1 nerve root is involved •Neurologic claudication may be present.
- 25. Asymptomatic Mild to Moderate Severe Correction of poor posture Elimination of stressful ccupation To avoid certain special sports activities Alleviation of anxiety Analgesics and muscle relaxants Deep heat exercises Rest NSAIDs Gradual Exercises Different methods of conservative treatment
- 26. Surgical Management Indications • Failure of conservative therapy. • Signs of root compression. • Progressive slipping. • Slip of more than 30 per cent even when painless • Persistent pain in the back, thigh or persistent sciatica. Methods of Surgery Posterolateral fusion Posterior fusion Laminectomy and intertransverse fusion Anterior interbody fusion.
- 27. Fig. 17.40: Posterior spinal stabilisation by Steffee plate and screws
- 28. Here patient complains of chronic backache, early morning stiffness, difficulty in getting out of bed, standing, sitting or climbing. The facet joint osteoarthritis (Arthroses of the facet joints) due to repeated bending and twisting activities lead to arthritis of facet joints. The crunch in the spine at movements Reduction pain after warm-up (gymnastics) Restriction of rotation in a lumbar spine The reason- monotonous work Kyphosis in the lumbar spine Rigidity in the spine Reduction pain after rest Signs
- 29. Denervation the facet joint Transcutaneous ankylosis (artificial ankylosis) +/- +/- Manuel therapy Steroids local injection Treatment
- 30. LUMBAR CANAL STENOSIS cauda equina compression in which the lateral or anteroposterior diameter of the spinal canal is narrow with or without a change in the cross-sectional area. a. Central b. Lateral recesses c. Foraminal d. Far out
- 31. Cauda aquina claudication Ischaemic claudication • Pain in buttocks and lower extremities after walking. • Pain in the legs appears on walking • Relieved by sitting forward for 20 minutes • Appears and diappears fast • Hyperesthesia, paraesthesia precipitated by walking, walking uphill, cycling etc. • No neurological deficit • Absent pulses • Pulses are felt • Trophic changes in footand toes i • No trophic changes. LUMBAR CANAL STENOSIS Stoop teat It is positive in lumbar canal stenosis. Ask the patient to walk briskly → pain develops → continues to walk → patient assumes a stooped posture → symptoms disappear. The pain decreases by forward bending because the canal length increases by 2.2 mm Difference Difference
- 32. Investigations Radiographs 1. Reduced interpedicle distance. 2. AP or midsagittal diameter of the affected vertebra (Normal—15 mm). 3. Measurement of the lateral sagittal diameter. 4. Hypertrophy and sclerosis of the facet joints. 5. Reduced interlaminar space and short, stout spinous process. 6. Associated features like presence of listhesis, prolapsed disc, osteophytes, etc. Myelography MRI and CT scan Help to diagnose lateral recess stenosis, facet hypertrophy, midsagittal distance, etc. Surgical Methods - surgical decompression.
- 33. Lumbar spondylosis Osteophytes In the elderly age group Self-stabilization motive segments of spine (RSH) Decrease height of disc