Including Mental Health Support in Project Delivery, 14 May.pdf
DKA algorithm Finalized - AT LAST.pptx
1. 3a
i
.
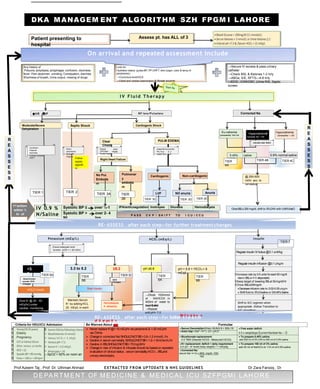
Prof Azeem Taj , Prof. Dr. Uthman Ahmad EXTRACTED FROM UPTODATE & NHS GUIDELINES Dr Zara Farooq , Dr
Mehreen
IV 0.9 %
N/Saline
Systolic BP ≤
90
over ½-1
hr
tPA/anticoagulation Inotropes Diuresis Hemodialysis
Systolic BP >
90
over 2- 4
hrs
R
E
A
S
S
E
S
S
Any history of
Polyuria, polydipsia, polyphagia, confusion, dizziness.
fever Pain abdomen, vomiting, Constipation, diarrhea
Shortness of breath, Urine output, missing of drugs
Look for:
Hydration status: (pulse,BP, PP,CRFT, skin turgor, color & temp of
peripheries)
→Conscious level/GCS
→Chest and cardiac examination & Bowel sounds
→Secure IV access & pass urinary
catheter
→Check BSL & Ketones 1-2 hrly
→ABGs, S/E, RFTS—4-8 hrly
→ECG , CXR/CBC ,Urine R/E, Septic
screen
Eu-natremia
CorrectedNa+
130-144
Corrected Na
OnceBSL≤ 200 mg/dl, shift to 5%D/W with 0.45%NaCl
R
E
A
S
S
E
S
S
0.9% normal saline
0.45%
(1/2
) saline
@ 250-500
ml/hr acc. to
vol status
Hypernatremia
Corrected Na+
> 145
Calculatewater deficit
Hyponatremia
CorrectedNa+
< 130
Warm
peripheries
Wide PP,
Oliguria
Follow
sepsis
algorith
m
Confusion
Postural
dizziness
Cramps Delayed
CRFT
Right Heart Failure
Pulmonar
y
embolis
m
No Pul.
Embolis
m
afeet
Raised
JVP.Edem
Tender Hepato
megaly
Clear
Chest
LVF
Non-cardiogenic
Cardiogenic
PULM EDEMA
SOB/ORTHO
PN Fine
CREPTS.N
EA/PN
D o
JVP
Anuria
NO anuria
HR ↓ BP BP less/Pulseless
Septic Shock Cardiogenic Shock
Moderate/Severe
Dehydration
1st action:
within ½
hr of
arrival
Potassium (mEq/L) Insulin
Regular insulin IVbolus @0.1 unit/kg
Regular insulin infusion @0.1 U/kg/hr
EIncrease rate by 0.5 units foreach50 mg/dl
rise in BSLor if it staysstatic.
EKeep target of lowering BSLat 50mg/dl/Hr
EOnce BSL≤200mg/dl:
Decreaseinfusion rate to 0.02-0.05u/kg/hr
Shift fluid to 5%D/salineor D/0.45%Saline
Shift to S/C regimen when
appropriate (follow Transition to
S/C algorithm)
HCO3
-(mEq/L)
→Dilute 100mmol
of NAHCO3 in
400ml of water to
be infused
over 2-4hr
→Repeat
NAHCO3
pH > 6.8 + HCO3 < 8
mEq/L
Give K+ @ 20 - 40
mEq/hr) under
cardiac monitoring
Maintain Serum
K+ by adding KCL
20 mEq/L in each
fluid)
Absent bowel
sounds ECG
Changes
ECG
Changes
Start Insulin
Hemodialysis
if refractory
3.3 to 5.2 ≥5.3
<3.
3
HOLD Insulin
Ensure adequate renal
function (UOP ≈ > 50 ml/hr)
Patient presenting to
hospital
Assess pt. has ALL of 3
On arrival and repeated assessment include
RE- ASSESS
P A S S C V P / S H I F T T O I C U / C C U
after each step—for further treatment changes
pH ≤6.8
Criteria for HDU/ICU Admission Be Warned About Formulae
E E
E Elderly o
E Pregnancy o
E o
E o
E o
E o SpO2 < 92% on room air
E
Never replace K+@>10 mEq/hr via peripheral & >20 mEq/hr
via CVline
Changein corrected Na+SHOULDNOTBE>0.8–1.2 mmol/L /hr
Decline in serum osmolality SHOULDNOTBE>1.2–1.8mOsm/L/hr
Decline in BSLSHOULDNOTBE>70mg/dl/hr
Changein rate of infusion & infusate should be basedon repeated
evaluation of clinical status , serum osmolality,HCO-
3 , BSLand
urinary electrolytes.
Serum Osmolality=2(Na)+ BUN/2.8 + BSL/18 Free water deficit:
0.5 x weight(kgs) (current Na/ideal Na – 1)
Anion Gap=(Na+ +K+)–(Cl- +HCO
-
)
Bicarbonate replacement:
0.5 TBW (Desired HCO3 - Measured HCO3)
To prepare 0.45% saline:
add 500 ml of 5% DW to 500 ml of 0.9% saline
K+ replacement: deficit + daily requirement
0.4 {(4 – K+ level) body weight} + 1 mEq/kg
To prepare 150 ml of 3% saline:
add 40 ml of NaHCO3 to 110 ml of 0.9% saline
Corrected Na:
serum Na+ +1.6 x (BSL mg/dl- 100)
100
DEPARTMENT OF MEDICINE & MEDICAL ICU SZFPGMI LAHORE
DKA MANAGEM ENT ALGORITHM SZH FPGM I LAHORE
TIER 1 TIER 2
TIER 3A TIER
3B TIER 3C TIER 3D TIER 3E
TIER
4A
TIER 4B TIER 4C
TIER 5A
TIER
5B
TIER 5C TIER
6A
TIER
6B
TIER 7
I V Fluid T herap y
until pH> 7.0
RE- ASSESS after each step—for further
B
e
t
C
r
a
e
u
t
a
i
o
t
u
m
s
of
e
S
n
er
t
um
c
K
h
+
anges