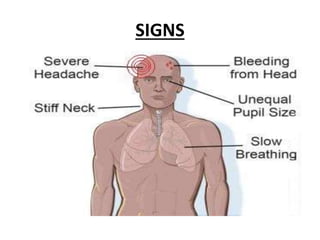
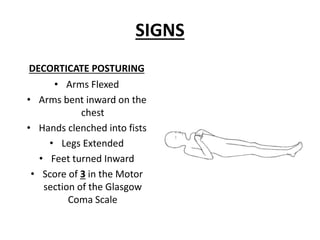
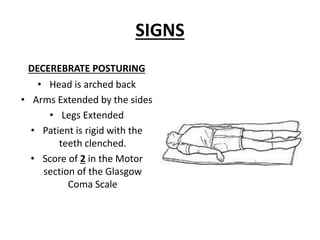
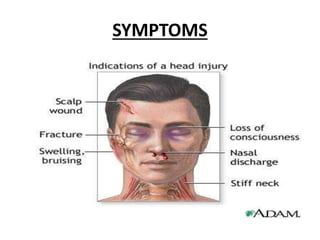
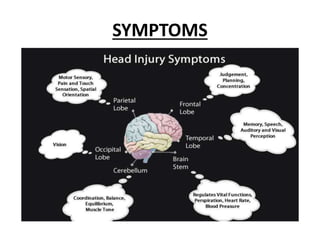
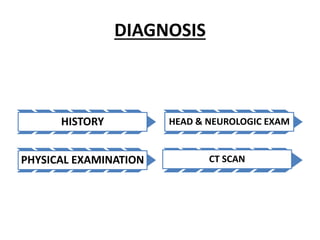
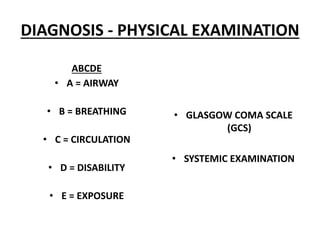
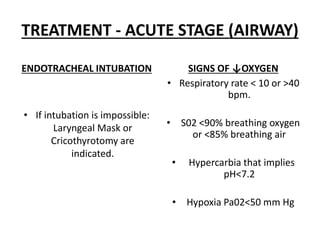
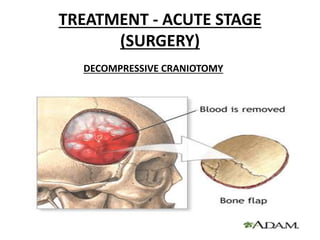
This document defines and describes head injuries, including types of injuries such as closed and open head injuries. It discusses mechanisms of primary and secondary brain injuries. It also outlines signs and symptoms, diagnosis including imaging tests, and treatment for both the acute and chronic stages. Treatment in the acute stage focuses on the ABCDE approach, increasing ICP management, and surgery if needed. Long term complications and prevention methods are also mentioned.
































































![Traumatic brain injury [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/traumaticbraininjuryautosaved-230313134042-a66a1551-thumbnail.jpg?width=640&height=640&fit=bounds)



























