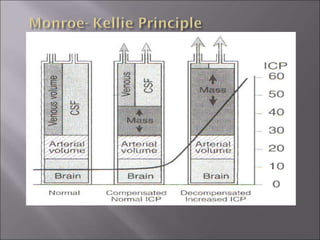
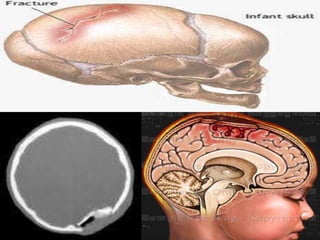
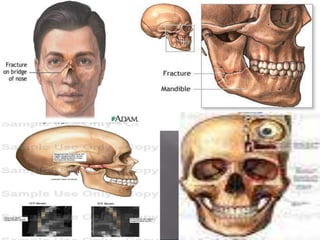
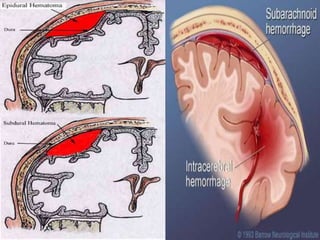
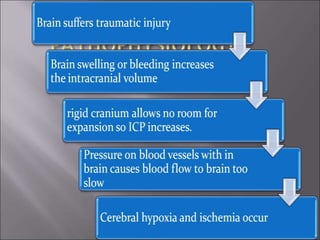
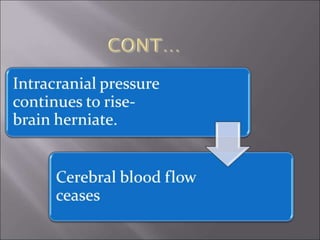
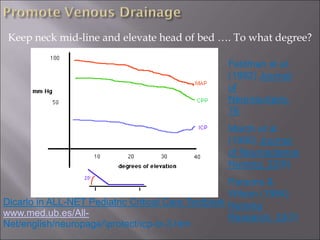
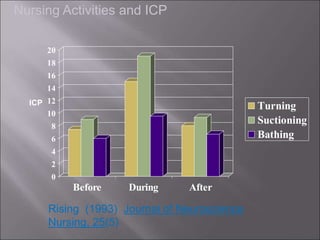
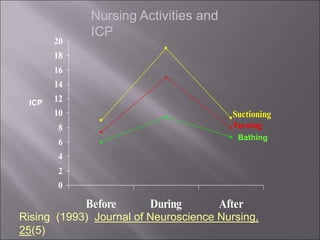
The document discusses various types of head injuries including concussion, contusion, and skull fractures, defines terms related to increased intracranial pressure, and outlines management of increased ICP including maintaining normal body temperature, administering medications to decrease ICP, and avoiding activities that could raise ICP like turning or suctioning.