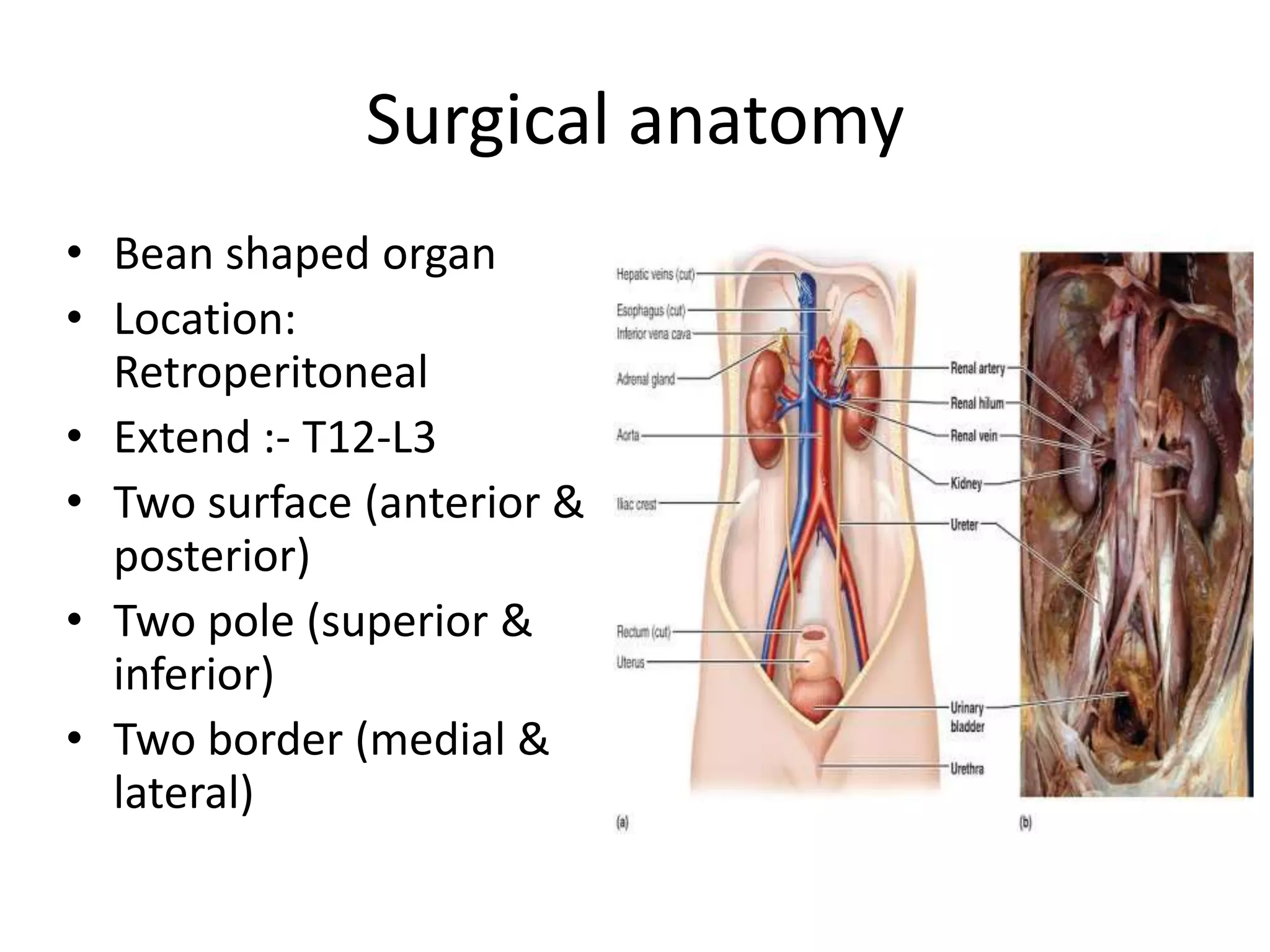
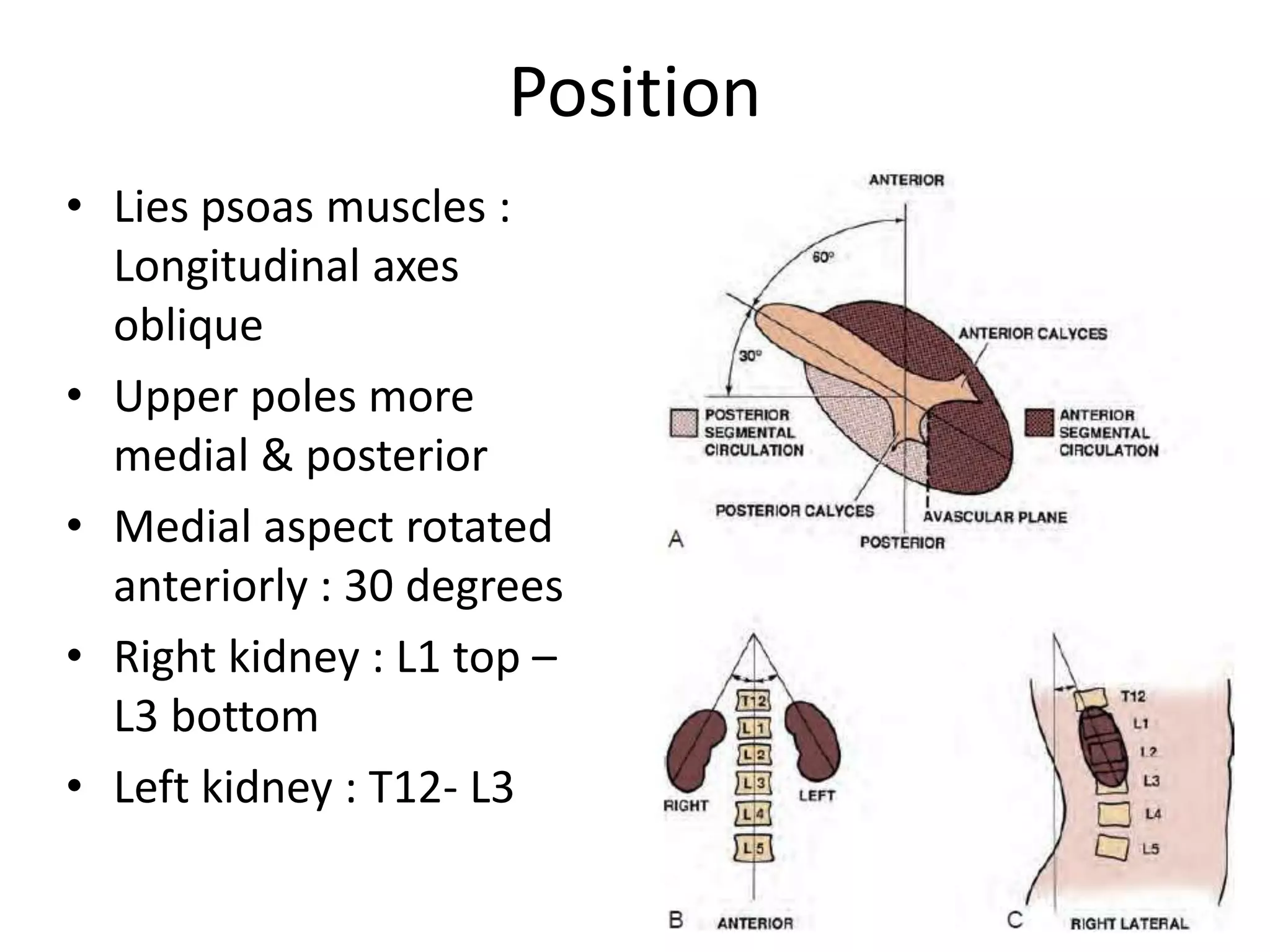
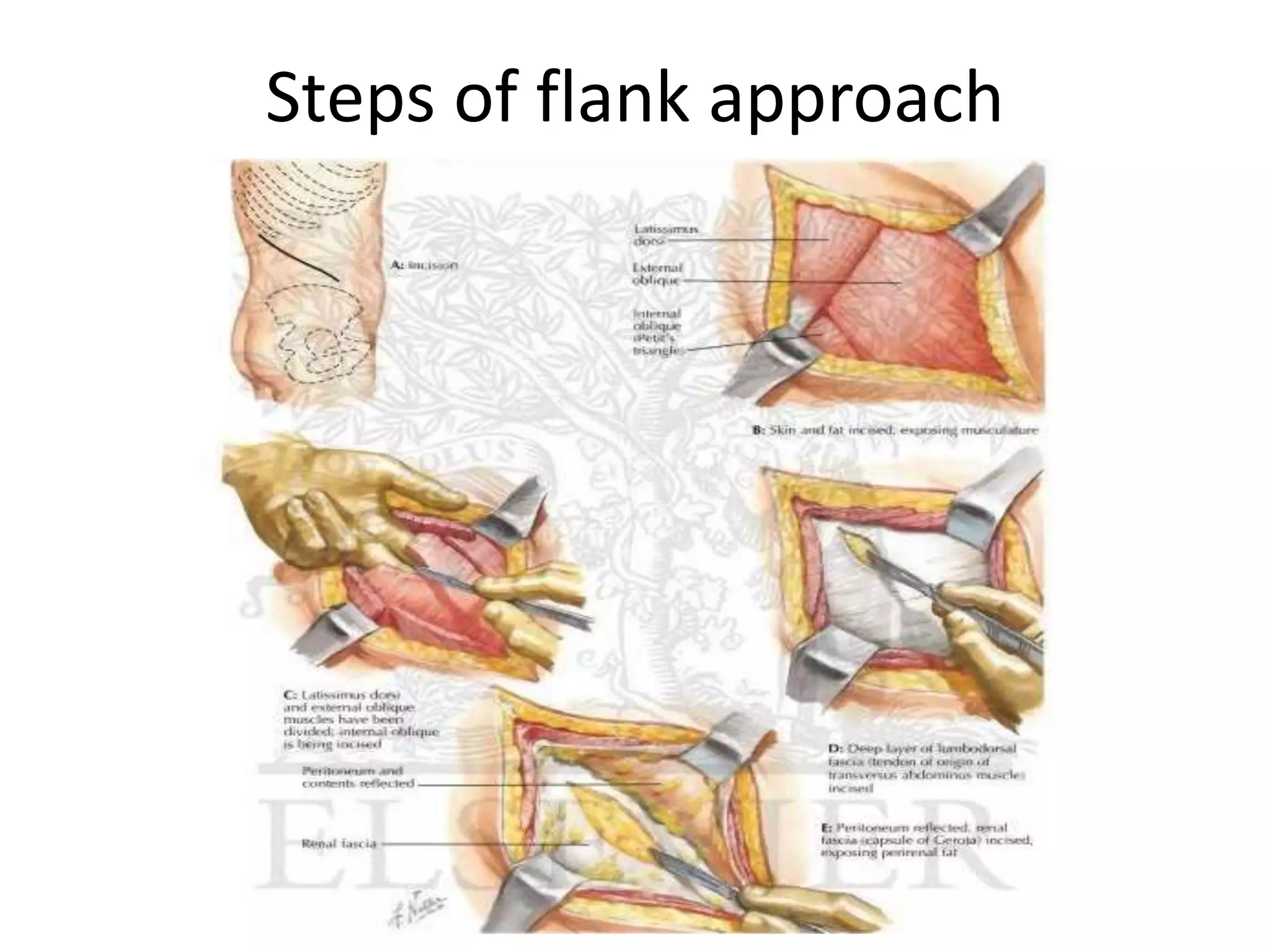
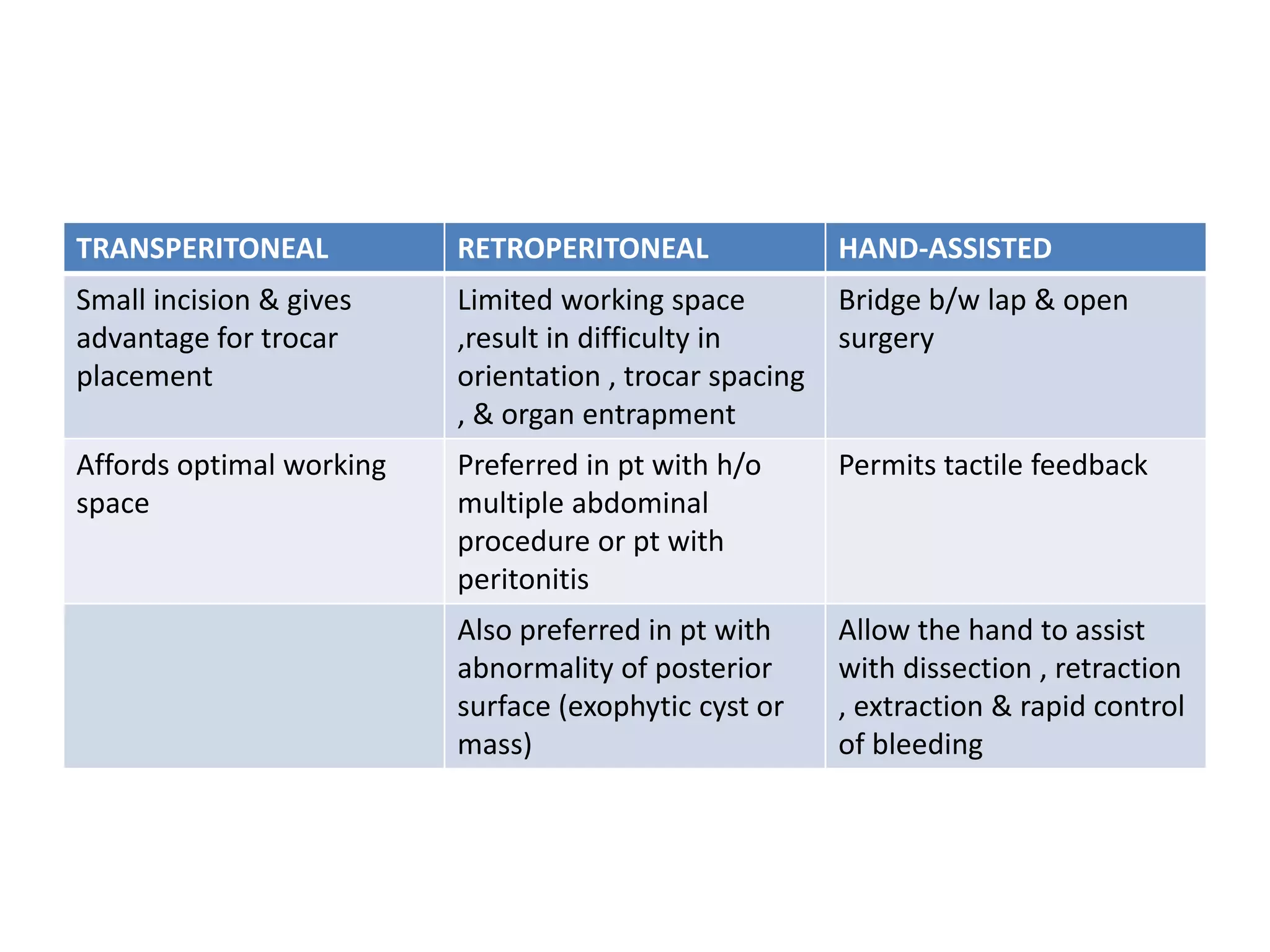
A nephrectomy is a surgical procedure to remove a kidney. There are several types including simple, partial, and radical nephrectomies. A surgeon must have knowledge of renal anatomy and vasculature. Approaches can be open, laparoscopic, or robotic. Key steps include mobilizing the kidney, isolating and ligating the renal vessels, and closing fascial layers. Complications include bleeding, fistula, and loss of renal function.