Download to read offline

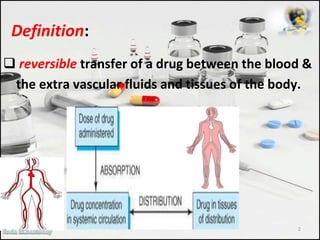




Volume of distribution (Vd) refers to the theoretical volume that a drug is distributed in the body. Vd is calculated as the dose administered divided by the drug concentration in plasma. A small Vd under 5L indicates distribution is mainly in plasma, while a large Vd over 41L means distribution is in tissues. Factors like molecular weight, pH, blood flow, and protein binding determine a drug's distribution. Drugs with high protein binding have a smaller Vd and longer duration since the bound fraction is unavailable for metabolism.



























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)







