Room to Breathe: Leveraging Biologic Agents and Multidisciplinary Care to Optimize Management in Chronic Rhinosinusitis With Nasal Polyps
•
0 likes•87 views

Chair, Jivianne T. Lee, MD, FACS, prepared useful Practice Aids pertaining to chronic rhinosinusitis with nasal polyps for this CME activity titled “Room to Breathe: Leveraging Biologic Agents and Multidisciplinary Care to Optimize Management in Chronic Rhinosinusitis With Nasal Polyps.” For the full presentation, downloadable Practice Aids, and complete CME information, and to apply for credit, please visit us at https://bit.ly/3OAVdSv. CME credit will be available until September 27, 2023.

Recommended
Recommended
More Related Content
Similar to Room to Breathe: Leveraging Biologic Agents and Multidisciplinary Care to Optimize Management in Chronic Rhinosinusitis With Nasal Polyps
Similar to Room to Breathe: Leveraging Biologic Agents and Multidisciplinary Care to Optimize Management in Chronic Rhinosinusitis With Nasal Polyps (20)
More from PVI, PeerView Institute for Medical Education
More from PVI, PeerView Institute for Medical Education (20)
Recently uploaded
Recently uploaded (20)
Room to Breathe: Leveraging Biologic Agents and Multidisciplinary Care to Optimize Management in Chronic Rhinosinusitis With Nasal Polyps
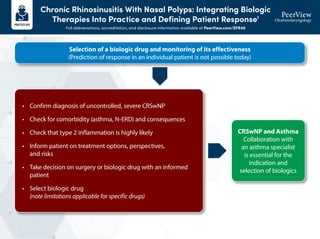
- 1. Chronic Rhinosinusitis With Nasal Polyps: Integrating Biologic Therapies Into Practice and Defining Patient Response1 Full abbreviations, accreditation, and disclosure information available at PeerView.com/ZFR40 Selection of a biologic drug and monitoring of its effectiveness (Prediction of response in an individual patient is not possible today) • Confirm diagnosis of uncontrolled, severe CRSwNP • Check for comorbidity (asthma, N-ERD) and consequences • Check that type 2 inflammation is highly likely • Inform patient on treatment options, perspectives, and risks • Take decision on surgery or biologic drug with an informed patient • Select biologic drug (note limitations applicable for specific drugs) CRSwNP and Asthma Collaboration with an asthma specialist is essential for the indication and selection of biologics
- 2. Chronic Rhinosinusitis With Nasal Polyps: Integrating Biologic Therapies Into Practice and Defining Patient Response1 Full abbreviations, accreditation, and disclosure information available at PeerView.com/ZFR40 1. Bachert C et al. J Allergy Clin Immunol. 2021;147:29-36. After 6 Months of Treatment After 12 Months of Treatment 6 12 Improvement of at least one symptom/score • Sense of smell: from anosmia to hyposmia/normosmia, smell score increase ≥0.5 • NCS: decrease by ≥0.5 or objective testing • NPS: decrease by ≥1 by nasal endoscopy • SNOT-22: reduction of ≥8.9 (minimal clinically important difference) • VAS total symptoms: reduction of ≥2 cm Adequate response (all of these definitions are fulfilled) • NPS <4 (total of both sides) • NCS <2 • VAS total symptoms <5 • SNOT-22 score <30 Further, there should be no current need for surgery or systemic GCS No No Yes Yes Improvement not acceptable to the patient Salvage surgery under biologic protection Stop – change to surgery or another biologic drug Consider another biologic drug Surgery Continue with biologic treatment Additional short course of systemic GCS Improvement acceptable to the patient Continue with biologic treatment Please note that these are expert consensus statements, not guidelines
- 3. The Advent of Targeted Biologic Therapy for CRSwNP Full abbreviations, accreditation, and disclosure information available at PeerView.com/ZFR40 1. Stevens WW et al. J Allergy Clin Immunol. 2016;4:565-572. 2. Patel GB et al. J Allergy Clin Immunol. 2020;8:1522-1531. 3. Dupixent (dupilumab) Prescribing Information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/761055s042lbl.pdf. 4. Xolair (omalizumab) Prescribing Information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/103976s5239lbl.pdf. 5. Nucala (mepolizumab) Prescribing Information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/761122s008,125526s019lbl.pdf. 6. Fokkens WJ et al. Allergy. 2019;74:2312-2319. Multidisciplinary Collaboration and Coordination6 PCP Otolaryngologist/ Rhinologist Allergist-Immunologist/ Pulmonologist Type 2 Biologic Therapies Approved for CRSwNP Omalizumab4 • Humanized mAb directed against IgE • Add-on maintenance treatment for nasal polyps in adults with inadequate response to intranasal corticosteroids Approved 2020 Dupilumab3 • Fully human mAb that inhibits signaling of IL-4 and IL-13 • Add-on maintenance treatment for adults with inadequately controlled CRSwNP Approved 2019 Mepolizumab5 • Humanized mAb targets and binds to IL-5 • Add-on maintenance treatment of adults with CRSwNP Approved 2021 CRSwNP Pathophysiology1,2 Allergens Particulates/ pollutants Viruses Proteases Airway epithelium Mast cell Adaptive response DC Th2 cell Eosinophilia Basophil M2 Goblet cell Eosinophil Cell recruitment Mucus response Remodeling B cell Th2 cell B cell IgE Mast cell LTC4 PGD2 IL-25R PGD2R (CRTh2, DP2) IL-33R (ST2) ILC2 cell IL-4 IL-5 IL-13 Type 2 cytokines TSLPR IL-25 IL-33 TSLP Type 2 inducers
- 4. CRSwNP Management: Multidisciplinary Consensus and EUFOREA Algorithms Full abbreviations, accreditation, and disclosure information available at PeerView.com/ZFR40 Management Algorithm Establish diagnosis and initial management Document subjective symptom severity Cardinal symptoms: Congestion, decrease in smell, drainage, facial pressure, and QOL measures Evidence of objective findings (Anterior rhinoscopy, nasal endoscopy, or CT) Start with intranasal steroid sprays ± consider short burst of oral steroids if not contraindicated EDS-FLU or Consider repeat, short bursts of oral steroids if not contraindicated Reassess symptom response and objective evidence of disease with at least 4 weeks of therapy With persistence of symptoms and evidence of disease, consider allergy testing, ASA challenge, CBC with differential, total IgE Multidisciplinary Consensus on a Stepwise Treatment Algorithm for Management of CRSwNP1
- 5. CRSwNP Management: Multidisciplinary Consensus and EUFOREA Algorithms Full abbreviations, accreditation, and disclosure information available at PeerView.com/ZFR40 Escalation of Treatment (If Refractory) Multidisciplinary Consensus on a Stepwise Treatment Algorithm for Management of CRSwNP1 (Cont’d) Majority of patients Sinus surgery (Discuss extent of surgery) Postoperative management Saline irrigation, steroid irrigation, INS, EDS-FLU, steroid sinus implant Minority of patients If symptoms persist or recur despite appropriate sinus surgery and postoperative topical steroid therapy (steroid irrigation, EDS-FLU, INS), consider comprehensive (multispecialty) approach for management (Shared decision-making process) Persistent disease Contraindication to surgery Poorly controlled asthma despite standard therapy/ OCS-dependent asthma Declined surgery (Shared decision-making process) Consider biologic (eg, dupilumab, omalizumab) Revision sinus surgery Steroid sinus implant Consider short burst of OCS Biologics for patients ± indicated comorbidities (eg, asthma) ASA desensitization for patients with AERD (if not contraindicated) Assess response in 6 mo Assess response in 6 mo
- 6. CRSwNP Management: Multidisciplinary Consensus and EUFOREA Algorithms Full abbreviations, accreditation, and disclosure information available at PeerView.com/ZFR40 1. Han JK et al. Int Forum Allergy Rhinol. 2021;110:1407-1416. 2. Fokkens WJ et al. Allergy. 2019;74:2312-2319. • Evidence of T2 inflammation • Need for systemic CS (≥2 courses in the past year) • Significantly impaired QOL • Significant loss of smell • Diagnosis of comorbid asthma History of surgery No history of surgery 3 Criteria required 4 EUFOREA Indications for Biologic Treatment of CRS/NP2 Bilateral nasal polyps