
Recommended
More Related Content
What's hot
Similar to Otitis media ear infection ppt
Similar to Otitis media ear infection ppt (20)
More from NehaNupur8
More from NehaNupur8 (20)
Recently uploaded
Recently uploaded (20)
Otitis media ear infection ppt
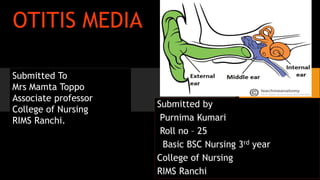
- 1. OTITIS MEDIA Submitted by Purnima Kumari Roll no – 25 Basic BSC Nursing 3rd year College of Nursing RIMS Ranchi Submitted To Mrs Mamta Toppo Associate professor College of Nursing RIMS Ranchi.
- 2. CONTENTS • Introduction • Classification • Acute otitis media • Otitis media with effusion • Chronic suppurative otitis media • Medical management • Surgical management • Complications • Prevention • Nursing management • Patient education • New research • Summary • Evaluation • Reference • Bibliography
- 5. Introduction • It is a middle ear infection. • Otitis means inflammation of the ear and media means middle. • Most often occur in infants and young children but can occur at any age. • Inflammation often begins with infection that cause sore throat , colds , other respiratory problems and spreads to the middle ear • Caused by virus or bacteria and can be acute or chronic
- 6. Definition Otitis media is inflammation of the middle ear or middle ear infection. • Otitis media is a general term refers to inflammation of the mucous membranes of the middle ear eustachian tube and mastoid
- 8. Classification 1. Acute otitis media 2. Otitis media with effusion 3. Chronic suppurative otitis media
- 9. Acute otitis media 1. Also known as suppurative otitis media or purulent otitis media. 2. It is an acute inflammation and infection of the middle ear mucosa. 3. Caused by pyogenic bacterial organisms which enter into middle ear via eustachian tube. 4. Usually rapid onset and short duration.
- 10. Etiology and risk factors • Bacterial eg . Streptococcus pneumoniae, Haemophilus influenzae, and moraxella species • Upper respiratory tract infection • Rhinovirus and respiratory syncytial virus • Prematurity and low birth weight • Family history and genetic predisposition • Deviated nasal septum and nasal polyps • Vitamin A , zinc and iron deficiency.
- 12. Pathology Stage of tympanic congestion Stage of exudation Stage of suppuration Stage of convalescence or recovery Stage of coalescent mastoiditis
- 13. Clinical manifestations • Sudden and severe earache ( otalgia) • Tinnitus • Hearing loss • Fever • Sense of fullness in ear • Irritability • Mastoid tenderness • Tympanic membrane erythema, may be perforated.
- 14. Diagnostic evaluation • History taking • Physical examination • Culture and sensitivity test • C T scan , MRI . • Audiometry and tympanometry • Nasopharyngoscopy
- 17. Management • Medical management 1. Antibiotic – Amoxicillin , Amoxicillin – clavulanate. 2. Analgesic • Surgical management 1. Myringotomy 2. Tympanocentesis
- 18. Myringotomy
- 19. Otitis media with effusion • Also know. as serous and secretory otitis media • It is simple a collection of fluid that occur within middle ear space as a result of the negative pressure produced by altered eustachian tube function. Causes • Viral URI • Bactetial infection • Acute otitis media. • Breast feeding in lying down
- 20. • Fluid in the middle ear sometimes causes conductive hearing impairment. • Fluid may become very thick and glue like.( Glue ear). Clinical manifestations • Non purulent effusion either mucoid or serous • Hearing losss • Aural fullness. Hearing loss is generally mild and is often detected only with an audiogram.
- 23. Treatment 1. Antimicrobial agents- Antibiotic such as erythromycin, sulfisoxazole, Amoxicillin, Amoxicillin clavulanate. 2. Surgery – Tympanocentesis , Laser myringotomy alternate to ear tube surgery.
- 24. Chronic suppurative otitis media • It is a chronic inflammation of the middle ear with tissue damage, usually caused by repeated episode of the acute otitis media • Develops after a prolonged period of time with fluid or negative pressure behind the tympanic membrane. • Perforated ear drum
- 26. Etiology • Inappropriate treatment of acute otitis media. • URTI, allergic rhinitis • Eustachian tube dysfunction • Adenoid hypertrophy and chronic sinusitis.
- 27. Classification 1. Tubotympanic type • Tubal type • Tympanic type 2. Atticoantral disease
- 30. Clinical manifestations • Persistent blockage of fullness of ear. • Hearing loss • Chronic foul smelling ear drainage • Vertigo • Facial weakness • Ear pain and headache • Fever • Tenderness of mastoid process • Middle ear mucosa is red edematous and swollen.
- 31. Diagnostic evaluation • Laboratory studies- culture and sensitivity of a specimen • Radiography • CT scan • MRI • audiogram
- 33. Medical management 1. Antibiotic – fluoroquinolones otic preparation with or without corticosteroid 2. Aural toilet 3. Control of granulation tissue – tropical antimicrobial drops 4. Treatment of underlying cause.
- 34. Surgical management 1. Myringoplasty 2. Myringotomy 3. Tympanoplasty 4. Ossiculoplasty 5. OtoLAM 6. Adenoidectomy 7. mastoidectomy
- 35. Complications Intra temporal • Mastoiditis • Petrositis • Facial paralysis • Labyrinthitis Intra cranial • Meningitis • Subdural abscess • Brain abscess • Lateral sinus thrombophlebitis
- 36. Prevention • Keeping a child away from Children with colds or upper respiratory tract infections • Not exposing the child to tobacco smoke • Feeding child in an upright position • Vaccine that protects pneumonia.
- 37. Nursing management • Assessment: • Collect health history includes a completedescription of the ear problem. • Collect data about the duration and intensity of the problem, its causes, and previous treatments. • Obtain Information about other health problems and medications. • Physical assessment includes observation for erythema, edema, otorrhea, lesions, and characteristics such as odor and color of discharge.
- 38. Nursing diagnosis 1. Pain related to inflammation and pressure on tympanic membrane 2. Risk for infection related to eustachian tube dysfunction 3. Impaired verbal communication related to hearing deficit 4. Altered auditory sensory perception related to middle ear infection 5. Fear and anxiety related to progression of disease.
- 39. Patient education • Teach patient or caregiver to administer ear medication. Drop should be administered at room temperature to avoid pain and dizziness. • Intruct patient or caregiver in safe techniques for cleaning ears. Thin washcloth and fingers are best for cleaning ears. • Instruct patient in the importance of routine examination by an audiologist
- 40. New research
- 41. Abstract Introduction: Chronic suppurative otitis media (CSOM) is a major health problem throughout the world in underdeveloped and developing countries including India The high prevalence of CSOM in school children in India has led us to undertake this study in school going children of rural and urban areas of Muzaffarnagar, Uttar Pradesh and to find out the various predisposing factors for the development of CSOM. Objectives: The objective is to find out the prevalence of CSOM in school going children of the rural and urban population about age, sex, and socioeconomic status Materials and Methods: Students were randomly selected from primary schools in rural and urban areas of Muzaffarnagar, Uttar Pradesh Cases selected was categorized in relation to age, sex, socioeconomic status, and prevalence of the safe and unsafe type of CSOM.
- 42. Observations: In the present study, a cross sectional survey was conducted in 2158 school children between the age group of 5 and 15 years. A total of 1161 children belonged to urban school whereas 997 children were from three adjacent rural government schools. A total of 78 children were found to be suffering from either unilateral or bilateral CSOM Conclusion: The prevalence of CSOM in urban school children was 2.32%, while for rural children, it was 5.11% .42.10% of cases of CSOM belonged to upper- lower socioeconomic group followed by lower middle group (31.57%). The tubotympanic disease was present in 87.18% of CSOM cases while 12.82% had atticoantral disease. Active CSOM was found amongst 37.18% while 62.82% had inactive disease. 42.10% had smoking father. 36 84% had indoor cooking with kerosene oil exposure, and 34.21% used unhygienic ear cleaning methods 31.58% had a history of recurrent URL 28.95% had chronic tonsillitis, and 21.05% of children had domain name system as associated findings with CSOM. Summary And Cancer ReferencesArt TubeRecommend this journal for your librarytitin
- 43. Summary
- 44. Evaluation • What is otitis media • Enlist type of otitis media • Describe acute otitis media . • What are the diagnosis evaluation of otitis media • What are the clinical manifestations of serous otitis media • What are the complications of otitis media • How you prevent otitis media. • Describe Nursing management of otitis media
- 45. Reference • Book • Internal • Discussion with teacher
- 46. Bibliography • Ansari Javed, textbook of medical surgical nursing, volume – 2, PV publications, page no- 34 to 36 • www.wikipedia.org • www.slidshare.net • www.indianjotol.org • www.google.com