Meniere's disease
•Download as PPTX, PDF•
16 likes•9,702 views

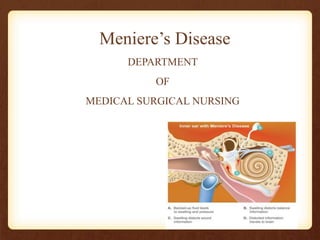
meniere disease is the inner ear condition which affect the patient haring and balance this ppt can help the nurses to take care of the patient affected with this disease and can be used as a study material for their examination

Recommended
More Related Content
What's hot
Similar to Meniere's disease
Similar to Meniere's disease (20)
More from Pallavi Lokhande
More from Pallavi Lokhande (20)
Recently uploaded
Recently uploaded (20)
Meniere's disease
- 2. Learning Objectives At the end of this lecturer, students should be able to: • Define meniere’s disease • List out the causes of Ménière’s Disease • Enumerate the clinical manifestation of Ménière’s Disease • Describe diagnostic evaluation of Ménière’s Disease • Explain the management of Ménière’s Disease
- 3. Definition • Meniers disease is a disorder of inner ear where the endolymphatic system is distended. It is chracterised by Virtigo, Sensorial hearing loss, Tinnitus and Aural fullness
- 4. Definition • Ménière’s disease is an abnormal inner ear fluid balance caused by a malabsorption in the endolymphatic sac. • Meniere ‘s disease is a disorder that affects the inner ear. That is responsible for hearing and balance • Evidence indicates that many people with Ménière’s disease may have a blockage in the endolymphatic duct.
- 6. Incidence • Male are affected more than female. • Disease is mainly unilateral. • It is more common in age group 35-60 years • About 50,000 - 100,000 people of world develop Meniere's disease in a year. • About 50 % of the patients who have Meniere's disease have a positive family history of this disease.
- 7. Causes • Unknown • Auto immune disease • Allergies • Endolymphatic hydrops • Either increased pressure in the system or rupture of the inner ear membranes occurs, producing symptoms of Ménière’s disease.
- 8. Risk factors • Toxicity (alcohol consumption ) • Head trauma • Smoking • Use of certain medication like asprin • Metabolic disorder (hypothyroidism) • Emotional factor (stress) • Anatomical abnormalities
- 9. pathophysiology Due to etiological causes Over production of endolymph Excessive accumulation in inner ear Increase pressure Rupture membrane Permanent loss auditory & vestibular function
- 10. Clinical Manifestations • fluctuating, loss of balance, headache • progressive sensorineural hearing loss; • tinnitus or a roaring sound; • a feeling of pressure or fullness in the ear; and episodic, • incapacitating vertigo, • nausea and vomiting.
- 12. Assessment and Diagnostic Findings • A careful history • Patients also complain of diaphoresis and • a persistent feeling of imbalance or disequilibrium, which may last for days. • During an acute attack, the patient has severe vertigo. Patients are sometimes diaphoretic and pale. Vital signs may show elevated blood pressure, pulse, and respiration.
- 13. • Weber test from a tuning fork. – lateralized to the better ear • Otoscopy • Audiometry • Electrocochleography • MRI, CT Scan
- 14. Complications • Inability to walk or function due to uncontrollable vertigo. • Hearing loss on the affected side. • Possible of injury due to imbalance. • Trauma from fall • Decrease quality of life
- 15. Medical Management • low-sodium (2,000 mg/day)diet. • Reassurance and bed rest • Psychological evaluation • Antihistamines such as meclizine • Tranquilizers such as diazepam • Antiemetics such as promethazine • Diuretic therapy (eg, hydrochlorothiazide)
- 16. Treatment summary 1. Atropine: stop attack for 20-30 Minutes 2. Bed rest in quite environment 3. Labyrinthine sedative like: Prochlorperazine (stemetil), Idmenhydrinate (Dramamine) to control giddiness and N/V 4. Vasodilators: Nicotinic acid, betahistamine to control vasospasm
- 17. 5. Tranquilizer and anti-depressant to relieve anxiety 6. Prphylactic antihistamine or mild sedative: Phenobarbitone, diazepam may be helpful. 7. Steroid to reduce inflamation 8. Antibiotics: esp. Aminoglycocise groups
- 18. SURGICAL MANAGEMENT •Endolymphatic Sac Decompression. •Endolymphatic sac decompression, or shunting. •Middle and Inner Ear Perfusion. •Intraotologic Catheters. •Vestibular Nerve Section.
- 19. Nursing management • Assessment History collection and physical examination • Nursing diagnosis • Imbalance nutritional status less than body requirement related to vomiting and fluid loss • Risk for injury related to disequilibrium or vertigo • Risk for Fluid volume deficit related to altered intake • Anxiety related to change health status and confusion
- 20. Altered auditory sensory perception related to altered state of the ear • Intervention • Assess the severity and frequency of attack, any associated ear symptoms (hear loss, tinnitus). • Help patient prevent from aura, so patient has time to prepare for an attack. • Encourage patient to lie down during attack in safe place. • Put side rails in the bed if patient is in bed • Place pillow to restrict movement.
- 21. Check vital sign Maintain patients fluid balance Monitor patient hearing activity Provide psychological support Provide medication as per doctor prescription Administer or teach anti-vertiginous medication and sedation medication as prescribed Avoid noises and glary bright light which may initiate attack. Advise patient to avoid food that cause allergy. Assist with ambulation when indicated. Provide comfort measures and avoid stress producing activities.
- 22. Post operative instructions: • Antibiotic and other medication are to be taken as prescribed. • Nose blowing to be avoided (few weeks). • Sneezing and coughing should be done with the mouth open for a few weeks after surgery. • Heavy lifting, straining, and bending are to be avoided for a few weeks after surgery. • Minor discomfort is expected can relief by analgesic, excessive pain should be reported to surgeon.
- 23. • Some slightly bloody or serosanganious drainage from the ear is normal after surgery. • Excessive or purulent drainage should be reported to the surgeon. • The cotton ball in the ear can be changed as needed but not to touch or remove any packing from the external auditory canal. • Post auricular suture line should be cleaned and antibiotic oint. Applied twice daily. • The surgeon should consult for regular air travel. • Getting water in the operated ear must be avoided for 2 weeks after surgery.
- 24. • Dressing first open-3rd day Suture removal 10th day Head up 300 (3-10 days) Avoid: Chewing, sneezing, coughing etc Prevent water in ear: 6 weeks Never put oil in ear Hearing may be impaired for few months RT edema, blood, fluid • Observe complications: Facial nerve palsy (VII), brain abscess, meningitis etc • Avoid flying in air for 2 months • BIPP dressing (bismuth icthymol parafin paste) while doing mastoid surgery
- 25. Summary • So far we have discussed about Definition, causes & risk factors, clinical manifestation, diagnostic evaluation and management of meniere's disease.
- 26. Bibliography • Lewis et al, Medical Surgical Nursing, Mosby Elsevier,7th edition. • Joyce.M.Black et al, Medical Surgical Nursing, Saunders publication. • Brunner and Siddhartha, Medical Surgical Nursing, Lippincott Williams and Wilkins.
- 27. Thank You