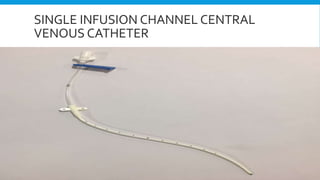
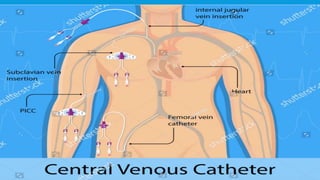
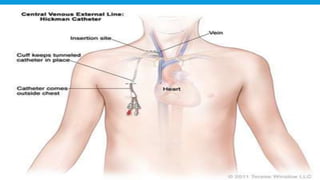
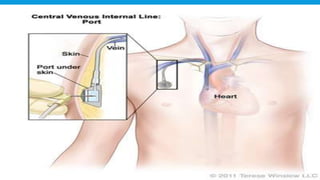
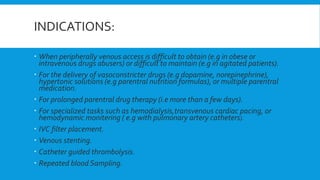
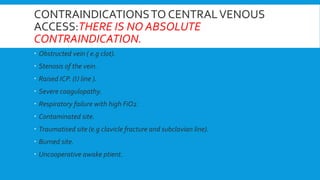
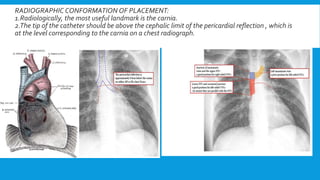
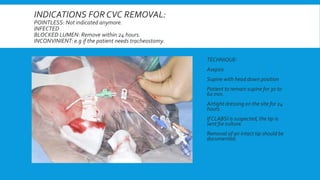
Central lines are catheters placed in large veins to allow delivery of fluids, drugs, and blood draws. They have multiple ports and are longer than typical IV lines. The document discusses types of central lines including PICCs, subclavian, internal jugular, and femoral lines. It describes parts of central lines and provides details on indications, site selection, insertion procedure including sterile precautions, positioning, and confirmation of proper placement. Potential complications are also summarized.