
Recommended
More Related Content
What's hot
What's hot (20)
Similar to DIAGNOSTIC TESTS FOR GASTROINTESTINAL SYSTEM.pdf
Similar to DIAGNOSTIC TESTS FOR GASTROINTESTINAL SYSTEM.pdf (20)
More from JishaSrivastava
More from JishaSrivastava (10)
Recently uploaded
Recently uploaded (20)
DIAGNOSTIC TESTS FOR GASTROINTESTINAL SYSTEM.pdf
- 1. HEALTH ASSESSMENT OF GASTRO INTESTINAL SYSTEM AND DIAGNOSTIC ASSESSMENT OF GI SYSTEM MRS. JISHA SRIVASTAVA, FACULTY RAKCON  1
- 2. TEXT OBJECTIVES  2 LEARN THE STRUCTURES AND FUNCTIONS OF THE GASTROINTESTINAL TRACT AND OF THE ACCESSORY GLANDS: LIVER, GALLBLADDER, AND PANCREAS LEARN AGE AFFECT ON THE GASTROINTESTINAL TRACT AND ACCESSORY GLANDS. LEARN THE TECHNIQUES USED IN PHYSICAL EXAMINATION OF THE ABDOMEN CONDUCTED FOR A PATIENT WITH POSSIBLE GASTROINTESTINAL SYSTEM, LIVER, GALLBLADDER AND PANCREATIC DISEASE. LEARN THE DIAGNOSTIC TESTS FOR THE DISORDERS OF THE GASTROINTESTINAL SYSTEM, LIVER, GALLBLADDER AND PANCREAS. LEARN TO DIFFERENTIATE NORMAL AND ABNORMAL FINDINGS. LEARN THE NURSING INTERVENTIONS FOR DIAGNOSTIC TESTS FOR THE DISORDERS OF THE GASTROINTESTINAL SYSTEM, LIVER, GALLBLADDER AND PANCREAS.
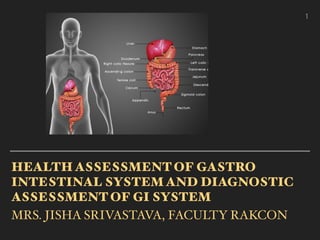
- 3. TEXT ANATOMY AND PHYSIOLOGY OF GI SYSTEM 1.ORAL CAVITY AND PHARYNX 2. ESOPHAGUS 3. STOMACH 4. SMALL INTESTINE 5. LARGE INTESTINE 6. LIVER 7. GALLBLADDER 8. PANCREAS  3
- 4. TEXT 1. ORAL CAVITY The boundaries of the oral cavity are the hard and soft palates superiorly, the cheeks laterally, and the floor of the mouth inferiorly. Within the oral cavity are the teeth and tongue and the openings of the ducts of the (salivary glands -parotid, submandibular, and sublingual glands).  4
- 5. TEXT 1. ORAL CAVITY The tongue is made of skeletal muscle innervated by the hypoglossal nerve (twelfth cranial nerve). The papillae on the upper surface of the tongue contain taste buds, innervated by the facial and glossopharyngeal nerves (seventh and ninth cranial).  5
- 6. TEXT The pharynx is a muscular tube that is a passageway for food exiting the oral cavity and entering the esophagus. When a mass of food is pushed backward by the tongue, the constrictor muscles of the pharynx contract as part of the swallowing reflex. This reflex is regulated by the medulla and pons. 1. ORAL CAVITY  6
- 7. TEXT 2.ESOPHAGUS The esophagus is about 10 inches long and carries food from the pharynx to the stomach. Peristalsis of the muscle layer in the wall of the esophagus is one way; food reaches the stomach even if the body is upside down.  7
- 8. TEXT 2.ESOPHAGUS The esophagus is surrounded by the lower esophageal sphincter (LES, or cardiac sphincter), a circular smooth muscle. The LES relaxes to permit food to enter the stomach and then contracts to prevent the back-up of stomach contents Incomplete closure of the LES may allow gastric juice to splash up into the esophagus.  8
- 9. TEXT 3. STOMACH The stomach is in the upper left abdominal quadrant, to the left of the liver and in front of the spleen. It is a J-shaped, saclike organ that extends from the esophagus to the duodenum of the small intestine. Some digestion takes place in the stomach, and it also serves as a reservoir for food so that digestion may take place  9
- 10. TEXT 3. STOMACH The fundus forms the upper curve of the stomach. The body of the stomach is the large, central portion, below that is antrum. The pylorus is adjacent to the duodenum, and the pyloric sphincter surrounds the junction of the two organs. When the stomach is empty, the mucosa has folds called rugae.  10
- 11. TEXT The mucosa contains gastric pits, the glands of the stomach that produce gastric juice. Gastric juice is mostly water and contains mucus, pepsinogen, hydrochloric acid, gastric lipase, and intrinsic factor. 3. STOMACH  11
- 12. TEXT 4. SMALL INTESTINE The small intestine is about 1 inch in diameter and approximately 10 feet long. The small intestine extends from the stomach to the cecum of the colon. The duodenum is the first 10 inches and contains the hepatopancreatic ampulla (ampulla of Vater), the entrance of the common bile duct and the pancreatic duct.  12
- 13. TEXT 5. LARGE INTESTINE The large intestine extends from the ileum of the small intestine to the anus. It is about 5 feet long and 2.5 inches in diameter. The cecum is the first part, and at its junction with the ileum is the ileo cecal valve, which prevents back-up of colon contents into the small intestine. Attached to the cecum is the small, dead-end appendix.  13
- 14. TEXT 6. LIVER The liver fills the right and center of the upper abdominal cavity. It has a larger right lobe and a smaller left lobe. The blood supply of the liver differs from that of other organs. The liver receives oxygenated blood by way of the hepatic artery.  14
- 15. TEXT 6. LIVER The only digestive function of the liver is the production of bile by the hepatocytes (liver cells). Bile flows through small bile ducts, converges into larger ones, and leaves the liver by way of the common hepatic duct.  15
- 16. TEXT CARBOHYDRATE METABOLISM. AMINO ACID METABOLISM. LIPID METABOLISM. SYNTHESIS OF PLASMA PROTEINS. PHAGOCYTOSIS BY KUPFFER CELLS. FORMATION OF BILIRUBIN. STORAGE DETOXIFICATION. ACTIVATION OF VITAMIN D AND K. 6. LIVER  16
- 17. TEXT 7. GALLBLADDER The gallbladder is a muscular sac about 3 to 4 inches long located on the undersurface of the liver. Bile in the common hepatic duct from the liver flows through the cystic duct into the gallbladder, which stores bile until it is needed in the small intestine. The gallbladder also concentrates bile by absorbing water.  17
- 18. TEXT The pancreas is about 6 inches long, and is located posterior to the greater curvature of the stomach. The digestive secretions of the pancreas are produced by exocrine glands called acini. The small ducts of these glands unite to form larger ducts and finally converge into the pancreatic duct, which joins the common bile duct to enter the duodenum at the hepatopancreatic ampulla. 7. PANCREAS  18
- 19.  19
- 21. TEXT 1. HEALTH HISTORY GI SYMPTOMS ‣ PAIN ‣ EXPOSURE TO CHEMICALS SUCH AS PAINT, FUMES, INDUSTRIAL DYES, ACIDS PESTICIDES TOXIC SUBSTANCES. STRESSORS  21 TRAVEL HISTORY ‣ DEMOGRAPHIC DATA ALCOHOL ABUSE/ TOBACCO CHEWING/ SMOKING/ USE OF OTHER RECREATIONAL DRUGS DISCOMFORT IN FOOD INTAKE, PAIN IN SWALLOWING BLOOD TRANSFUSIONS OR BLOOD PRODUCTS DENTAL PROCEDURES, BODY PIERCING OR TATTOOING PRE-EXISTING DISEASE
- 22. TEXT 1. HEALTH HISTORY ‣ LIVER OR GALLBLADDER DISEASE MAY HAVE PALE OR CLAY COLOURED STOOLS. ‣ EVIDENCE OF FOUL SMELL, FAT, PUS, BLOOD, OR MUCUS IN STOOL  22 BLOODY OR TARRY STOOLS, RECTAL BLEEDING, ABDOMINAL PAIN PATIENT’S NORMAL BOWEL PATTERN AND CHANGES IN BOWEL PATTERNS OR HABITS. ULCERS, CANCER, CROHN’S DISEASE, OR COLITIS; OR AN UNEXPLAINED WEIGHT LOSS OR GAIN. MOUTH ULCERS
- 23. TEXT 1. HEALTH HISTORY ABDOMINAL DISTENTION IN THE PRESENCE OF NAUSEA AND VOMITING MAY INDICATE INTESTINAL OBSTRUCTION. ‣ PATIENTS WITH LIVER, GALLBLADDER, OR PANCREATIC DISEASE MAY ALSO COMPLAIN OF FEELING BLOATED, OF HAVING GAS OR BELCHING FREQUENTLY, OR OF RIGHT UPPER QUADRANT (RUQ) TENDERNESS. PREVIOUS GI SURGERIES PREVIOUS DIAGNOSTIC TESTS  23 ‣ THE TOXINS PRODUCED BY C. DIFFICILE CAN CAUSE DIARRHEA, COLITITS, TOXIC MEGACOLON, DEHYDRATION, COLONIC PERFORATION, AND SOMETIMES DEATH.
- 24. TEXT 2. MEDICATIONS ‣Non- steroidal anti- inflammatory drugs (NSAIDs), aspirin, vitamins, laxatives, enemas, or antacids. Elderly patients may use laxatives regularly and develop a dependence on them. Over the counter preparations and herbal or natural products Medications are being taken with or without a physician’s prescription.  24
- 25. TEXT 3. NUTRITIONAL ASSESSMENT  25 A DIET HISTORY SHOULD INCLUDE USUAL FOODS AND FLUIDS, ALLERGIES, APPETITE PATTERNS, SWALLOWING DIFFICULTY, AND USE OF NUTRITIONAL AND HERBAL SUPPLEMENTS ACID REFLUX CAN BE ASSESSED BY ASKING PATIENTS IF THEY EXPERIENCE REFLUX WITH A BILE TASTE OR AWAKEN WITH AN UNPLEASANT TASTE IN THEIR MOUTH. ABNORMAL WEIGHT LOSS OR UNEXPECTED WEIGHT GAIN CHANGES IN FOOD TOLERANCE, INCLUDING THE TYPE OR AMOUNT OF OFFENDING FOODS
- 26. TEXT 3. NUTRITIONAL ASSESSMENT  26 PATIENTS WITH GALLBLADDER DISEASE MAY REPORT THAT THEY FEEL NAUSEATED OR BLOATED AFTER EATING FRIED INDIGESTION, HEARTBURN, NAUSEA, VOMITING, DIARRHEA, CONSTIPATION, FLATULENCE INCONTINENCE, ALL OF WHICH MAY INTERFERE WITH PROPER NUTRITION. PATIENTS WITH DISEASE OF THE LIVER, PANCREAS, OR GALLBLADDER COMMONLY HAVE CHANGES IN APPETITE SUCH AS ANOREXIA OR ALTERATIONS IN EATING PREFERENCES. THE ELDERLY PATIENT’S DAILY FOOD INTAKE SHOULD BE EXPLORED
- 27. TEXT 4. FAMILY HISTORY Family history of close relatives with conditions that may influence the patient’s GI status is assessed. Some GI problems such as colon cancer are thought to be hereditary. The patient’s history should note whether there is a family history of liver, pancreas, or gallbladder diseases, such as diabetes mellitus, alcoholism, cancer, heart disease, or bleeding tendencies. These diseases have a high incidence within families.  27
- 28. TEXT 5. CULTURAL INFLUENCES 1. ARABS MANY ARABS EAT FOOD ONLY WITH THEIR RIGHT HAND BECAUSE IT IS REGARDED AS THE CLEAN HAND. THE LEFT HAND, COMMONLY USED FOR TOILETING, IS CONSIDERED UNCLEAN. MUSLIM ARABS MAY REFUSE TO EAT MEAT THAT IS NOT HALAL 2. ASIAN INDIAN BERIBERI (THIAMINE DEFICIENCY) IS FOUND IN PEOPLE EMIGRATING FROM RICE-GROWING AREAS. PELLAGRA (NIACIN DEFICIENCY), CAUSING SKIN AND MENTAL DISORDERS AND DIARRHEA, IS FOUND IN PEOPLE EMIGRATING FROM MAIZE-MILLET AREAS. THIAMINE DEFICIENCY IS COMMON AMONG PEOPLE MOSTLY DEPENDENT ON RICE.  28
- 30. TEXT 1. HEIGHT, WEIGHT, AND BODY MASS INDEX When the GI system is assessed, the patient’s height and weight are obtained for planning care. The patient’s ideal body weight according to height is obtained using current reference charts.  30
- 31. TEXT 1. HEIGHT, WEIGHT, AND BODY MASS INDEX BMI Categories: Underweight <18.5 Normal weight 18.5–24.9 Overweight 25–29.9 Obesity is BMI of 30 or greater Excess waist circumferences (for women, more than 35 inches; for men, more than 40 inches) place people at greater risk for diabetes and cardiovascular disease.  31
- 32. TEXT ASSESSMENT OF ORAL CAVITY ‣ ≈ Gastrointestinal assessment begins with the oral cavity. The lips are examined for lesions, abnormal colour, and symmetry. With a penlight and tongue blade, the oral cavity is inspected for inflammation, tenderness, ulcers, swelling, bleeding, and discolouration. Any odour of the patient’s breath is noted. A foul odour may indicate infection or poor oral care. The tongue should be pink with a rough texture and assessed for signs of dehydration such as dryness, cracks, or furrows. The patient’s gums should be pink without swelling, redness, or irregularities.  32
- 33. TEXT ASSESSMENT OF ORAL CAVITY The teeth or dentures are examined for loose, broken, or absent teeth and the fit of the dentures or dental work. Ill-fitting dentures can affect the patient’s nutritional intake and obstruct the airway. Loose teeth can become dislodged and aspirated into the airway. Broken teeth can be a source of pain and contribute to poor nutritional intake. The ability of the patient to perform oral care is noted and included in the plan of care if there are deficits. ulcers, sores, or tender areas in the mouth that won’t heal after a week or two  33
- 34. TEXT ASSESSMENT OF ORAL CAVITY Bleeding or swollen gums after brushing or flossing Chronic bad breath Sudden sensitivity to hot and cold temperatures or beverages Pain or tooth ache, loose teeth Receding gums Pain with chewing or biting Swelling of the face and cheek Clicking of the jaw  34
- 36. TEXT 1. ABDOMEN INSPECTION. To inspect the abdomen, patients are placed in a supine position with their arms at their sides. The contour may be rounded, flat, concave, or distended, depending on the patient’s body type. Irregularities in contour may be due to distention, tumors, hernia, or previous surgeries Abdominal pulsatile masses are noted, they may be visible in thin persons or they may indicate an abdominal aortic aneurysm.  36
- 37. TEXT The bluish discoloration of the umbilicus (Cullen's sign) or flanks (Grey Turner's sign). 1. ABDOMEN INSPECTION.  37
- 38. TEXT Inspect the patient’s skin for bruising, caput medusa (bluish purple swollen vein pattern extending out from the navel), and spider angiomas (thin reddish purple vein lines close to the skin surface). The skin should be inspected for striae, or "stretch marks," and surgical scars. 1. ABDOMEN INSPECTION.  38
- 39. TEXT Note any petechiae, visible movement or peristalsis, or jaundice (also called icterus, a yellowing of the skin and the sclerae of the eyes). Jaundice is a cardinal symptom of liver or gallbladder disease and red blood cell disorders. Urine becomes dark, and if bile flow to the bowel is obstructed, stools will be a light clay color. 1. ABDOMEN INSPECTION.  39
- 40. TEXT 2. AUSCULTATION. When auscultating the patient’s abdomen, the upper right quadrant is auscultated first. Then a clockwise direction is followed to listen to the other quadrants. The stethoscope is pressed lightly on the abdomen to listen for bowel sounds, which are soft clicks and gurgles that may be heard every 5 to 15 seconds, occurring irregularly 5 to 30 times per minute.  40
- 41. TEXT 2. AUSCULTATION. Bowel sounds are produced when peristalsis moves air and fluid through the GI tract and are categorised as normal, hyperactive, hypoactive, or absent. Bowel sounds are considered absent if no sounds are auscultated after listening to all four quadrants for 2 to 5 minutes in each quadrant. Abdominal surgery.  41
- 42. TEXT 2. AUSCULTATION. Hyperactive bowel sounds are usually rapid, high pitched, and loud and may occur with hunger or gastroenteritis. Hypoactive bowel sounds are bowel sounds that are infrequent and can occur in patients with a paralytic ileus or following surgery. With a bowel obstruction, a high-pitched tinkling sound that is proximal to the obstruction. Auscultation for abdominal bruits is the next phase of abdominal examination. Bruits are "swishing" sounds heard over major arteries during systole . The area over the aorta, both renal arteries. and the iliac arteries should be examined carefully for bruits.  42
- 43. TEXT 3. PERCUSSION. Percussion produces a sound that identifies the density of the organs beneath and is performed by the physician or advanced nurse practitioner. Percussion is used to detect fluid, air, and masses in the abdomen and to identify size and location of abdominal organs (especially the liver and spleen). Tympanic high-pitched sounds indicate the location of air, and dull thuds indicate fluid or solid organs. Palpation and percussion are used to evaluate ascites. A rounded, symmetrical contour of the abdomen with bulging flanks is often the first clue.  43
- 44. TEXT 3. PERCUSSION. Palpation of the abdomen in the patient with ascites will often demonstrate a doughy, almost fluctuant sensation. In advanced cases the abdominal wall will be tense due to distention from the contained fluid. Gas-filled intestines will float to the top of the fluid-filled abdomen. Thus, in the supine patient with ascites there should be periumbilical tympany with dullness in the flanks. A change in the level of dullness is termed shifting dullness and usually indicates more than 500 ml of ascitic fluid. Another physical sign of ascites is demonstration of a transmitted fluid wave. The patient or an assistant presses a hand firmly against the abdominal wall in the right and tapped from left if a thrill present, it shows fluid.  44
- 45. TEXT 3. PERCUSSION.  45 The examiner places the flat of the left hand on the right flank and then taps the left flank with his right hand. In the presence of ascites, a sharp tap will generate a pressure wave that will be transmitted to the left hand. Unfortunately, fat will also transmit a fluid wave, and there are frequent false-positives with this test. In addition to detection of ascites, percussion can be used to help define the nature of an abdominal mass. Tympany of an abdominal mass implies that it is gas filled (i.e., intestine). Percussion is also used to define liver size. Abdominal girth is measured by placing a tape measure around the patient’s abdomen at the iliac crest. Abnormal or absent bowel sounds are important findings and should be documented and reported to the physician.
- 46. TEXT 4. PALPATION. Light palpation of the abdomen concludes the physical assessment. If the patient is having pain that area should be palpated last. Using the same quadrant approach as previously mentioned, lightly depress the abdomen not more than 0.5 to 1.0 inch during the palpation . Note any muscle tension, rigidity, masses, or expressions of pain. Deep palpation of the abdomen is done only by physicians and highly skilled nurses such as nurse practitioners. Daily measurements should be obtained and recorded to monitor changes when abdominal girth is abnormal. Abdominal girth is increased in patients with distention or conditions such as ascites (accumulation of fluid in the peritoneal cavity). The liver is not normally palpable, but if enlarged, it may be felt below the right lower rib cage. Rebound tenderness is determined by pressing down on the abdomen a few inches and quickly releasing the pressure.  46
- 47. TEXT 4. PALPATION. If the patient feels a sharp pain during this procedure, appendicitis may be indicated. Rigidity is thus a clear-cut sign of peritoneal inflammationRebound tenderness is the elicitation of tenderness by rapidly removing the examining hand. Spasm or rigidity is the involuntary tightening of the abdominal musculature that occurs in response to underlying inflammation.  47
- 48. TEXT 4. PALPATION. All that needs to be done is smoothly but quickly to lift the palpating hand off the abdomen and observe for pain, facial grimace, or spasm of the abdominal wall. palpation of the left lower quadrant may produce tenderness and rebound tenderness in the right lower quadrant in appendicitis (Rovsing's sign). This is called referred tenderness and referred rebound. When abdominal masses are palpated, the first consideration is whether the mass is intra-abdominal or within the abdominal wall. This can be determined by having the patient raise his or her head or feet from the examining table. This will tense the abdominal muscles, thus shielding an intra- abdominal mass while making an abdominal wall mass more prominent. If the mass is intra-abdominal, important points are its size, location, tenderness, and mobility.  48
- 49. TEXT 4. RECTAL INSPECTION AND PALPATION The anal canal is approximately 2.5 to 4 cm (1 to 1.6 inches) in length and opens into the perineum. Concentric rings of muscle, the internal and external sphincters, normally keep the anal canal securely closed. Gloves, water- soluble lubrication, a penlight, and drapes are necessary tools for the evaluation. Positions for the rectal examination include knee-chest, left lateral with hips and knees flexed, or standing with hips flexed and upper body supported by the examination table. External examination includes inspection for lumps, rashes, inflammation, excoriation, tears, scars, pilonidal dimpling, and tufts of hair at the pilonidal area. The discovery of tenderness, inflammation, or both should alert the examiner to the possibility of a pilonidal cyst, perianal abscess, or anorectal fistula or fissure.  49
- 50. TEXT 4. RECTAL INSPECTION AND PALPATION The patient’s buttocks are carefully spread and visually inspected until the patient has relaxed the external sphincter control. The patient is asked to bear down, thus allowing the ready appearance of fistulas, fissures, rectal prolapse, polyps, and internal hemorrhoids. Internal examination is performed with a lubricated index finger inserted into the anal canal while the patient bears down. The tone of the sphincter is noted, as are any nodules or irregularities of the anal ring. Because this is an uncomfortable part of the examination for most patients, the patient is encouraged to focus on deep breathing and visualization of a pleasant setting during the brief examination.  50
- 53. TEXT DIAGNOSTIC STUDIES  53 LABORATORY TESTS IMAGING TESTS ENDOSCOPIC PROCEDURES OTHERS PROCEDURES
- 59. TEXT A. LACTOSE INTOLERANCE BREATH TEST The patients are given to drink a lactose heavy beverage Analyze patient’s breath at regular intervals to measure the amount of hydrgen. If the lactose is not digested by the body, it will be fermented by bacteria, leading to a production of various gases, including hydrogen. High levels of hydrogen in the breath indicate that the body cannot properly digest lactose  59
- 60. TEXT B. HELICOBACTER PYLORI (H. PYLORI) BREATH TEST The patient will be instructed not to eat or drink one hour before the test. The patient will be connected to a nasal breath cannula attached to a Breath Analyser. After measuring a baseline sample, The patient will be given a 5 ounce solution to drink. If H. pylori is present, CO2 will be released into the bloodstream and carried to the lungs where it will be released and electronically analyzed if H. pylori is present. Testing time is about 10 minutes.  60
- 61. C. FRUCTOSE INTOLERANCE BREATH TEST This test determines whether The patient have difficulty absorbing fructose, a sugar found in onions, artichokes, pears and wheat. It is also used as a sweetener in some drinks. If The patient have symptoms such as bloating, gas, cramping and diarrhea, it may be due to fructose malabsorption.This test is similar to the test for lactose. Analyze the breath for hydrogen gas after drinking a cup of fructose dissolved in water. We obtain more breath results for the next three hours. If there is a high presence of hydrogen, that indicates your body has difficulty absorbing the fructose.  61
- 62. TEXT D. BACTERIAL OVERGROWTH SYNDROME (SIBO) Bacteria growing uncontrolled in the small intestine can cause small intestine bacterial overgrowth (SIBO). The patient may experience excessive bloating, gas, cramping and diarrhea. The patient drink a sugar solution. Breathe into a breath analyser. If bacteria are fermenting in the patient small intestine, they will come out in the patient breath. The doctor can confirm a diagnosis of SIBO  62
- 64. TEXT A. FLAT PLATE OF THE ABDOMEN A flat plate of the abdomen is an x-ray examination giving an anterior-to-posterior view . Can detect tumors, obstructions, and strictures. For an x-ray examination, the patient should be dressed in a hospital gown without any metal such as zippers, belts, or jewelry. Pregnant patients or those thought to be pregnant should avoid x-ray examinations.  64
- 65. TEXT B. UPPER GASTROINTESTINAL SERIES (BARRIUM) It is an x-ray examination of the esophagus, stomach, duodenum, and jejunum using an oral liquid radiopaque contrast medium (barium) and a fluoroscope to outline the contours of the organs. The patient drinks the thick, chalky barium while standing in front of a fluoroscopic tube. X-ray films are taken in various positions and at specific intervals to visualize the outline of the organs and to note the passage of Detect strictures, ulcers, tumors, polyps, hiatal hernias, and motility problems. Cancer Esophageal varices Dysphagia ,Achalasia  65
- 66. TEXT B. UPPER GASTROINTESTINAL SERIES B. UPPER GASTROINTESTINAL SERIES (BARRIUM)  66 NURSING INTERVENTIONS NPO from midnight Avoid smoking, chewing gum and using mints because they can stimulate gastric motility Morning dose Oral medications should be withheld Follow up care after the procedure to ensure that the patient has eliminated most of the ingested barium Provide adequate fluids to facilitate evacuation of stool and barium A laxative is usually ordered after the procedure to expel the barium and prevent constipation or a barium impaction.
- 67. TEXT C.LOWER GASTROINTESTINAL SERIES (BARIUM) Tumors Diverticula Stenosis Obstructions Inflammation Ulcerative colitis Polyps can be detected.  67
- 68. TEXT C.LOWER GASTROINTESTINAL SERIES (BARIUM The lower GI series (barium enema) is performed to visualize the position, movements, and filling of the colon. The patient is placed on a low- residue or clear liquid diet for 2 days before the test to empty the bowel. Laxatives, bowel-cleansing solutions (such as GoLYTELY), and enemas may be administered the evening before the test. GoLYTELY is chilled and drunk full strength with no ice, 8 oz every 10 minutes for a total of 4 L. Inform the patient that a watery diarrhea will begin in about 1 hour and continue up to 5 hours as the bowel is cleared. This is necessary for adequate visualization during the  68
- 69. TEXT C.LOWER GASTROINTESTINAL SERIES (BARIUM) If the patient has active inflammatory disease of the colon or suspected perforation or obstruction, a barium enema is contraindicated. Active GI bleeding may also prohibit the use of laxatives and enemas. During the procedure, barium is instilled rectally and x- ray films are taken with or without fluoroscopy. The patient may experience some abdominal cramping and an urge to have a bowel movement during the procedure. The patient is told to take slow, deep breaths and to tighten the anal sphincter. The rate of flow of the barium is slowed until the cramping diminishes. The procedure takes about 15 minutes, and the patient is allowed to use the bathroom immediately  69
- 70. TEXT C.LOWER GASTROINTESTINAL SERIES (BARIUM Nursing interventions Preparation of patient includes emptying and cleansing the lower bowel Low residue diet 1 to 2 days before the test, a clear liquid diet and a laxative in the evening before, NPO after midnight and cleansing enemas until returns are clear the following morning The nurse ensures that barium enemas are scheduled before any upper GI studies Barium enemas are contraindicated if the patient has active inflammatory disease of the colon, or patients with signs of perforation or obstruction  70
- 71. TEXT D. COMPUTED TOMOGRAPHY Computed tomography (CT) uses a beam of radiation to allow three- dimensional visualization of abdominal structures. Diluted oral barium or other contrast media may be used to distinguish normal bowel from abnormal masses. The patient may have a clear liquid diet the morning of the test. If a contrast medium is to be used, any allergies to iodine or contrast media are noted, a consent form is signed, and the patient is NPO for 2 to 4 hours before the procedure.  71
- 72. TEXT D. COMPUTED TOMOGRAPHY Nursing interventions A CT scan is performed with or without oral or IV contrast, but the enhancement of the study is greater with the use of a contrast agent Any allergies to contrast agent, iodine or shell fish, the patients current serum creatinin level and pregnancy status in females must be determined before administration of an contrast agent Kidney protective measures include the administration of IV sodium bicarbonate 1 hour before and 6 hours after iv contrast and oral acetylcysteine (mucomist) before or after the study Hydrate the patient after the procedure to prevent renal failure  72
- 73. TEXT E. NUCLEAR SCANNING Nuclear scanning involves injecting a patient with a small amount of radioactive isotope. The scan may be called a cholescintigraphic, DISIDA, HIDA, or IDA scan, depending on the radioactive isotope and exact procedure that is used. Prior to the procedure, the patient fasts and does not chew gum for at least 2 to 6 hours. After the injection, the isotope is secreted into the bile and goes anywhere the bile goes. Visualization of these areas occurs about 60 minutes after the IV injection.  73
- 74. TEXT F. ANGIOGRAPHY Angiography may be ordered for patients with symptoms of arterial occlusive disease of the hepatic, biliary, and pancreatic arterial vessels. It is used to evaluate suspected neoplasms in these organs. Medications that might cause bleeding, such as aspirin, NSAIDs, or anticoagulants, are stopped about 1 week prior to the procedure. A contrast medium is injected and identifies abnormalities of vascular structure and function, masses, and show bleeding sites. Prior to the procedure, the patient usually is NPO for 2 to 8 hours. The injection of contrast medium is done about 1 hour before the examination. Radiographs are taken about every 20 minutes for 1 hour or until the structures are readily viewed. The radiopaque material is iodine based, so ask the patient about any allergies to iodine. Following the procedure, observe for bleeding at the puncture site.  74
- 75. TEXT Nursing interventions Ask if allergies to contrast media or iodine. NPO for 2–8 hours prior to test. Stop medications that interfere with clotting about 1 week prior to exam. Assess for bleeding and hematoma formation after the exam. F. ANGIOGRAPHY  75
- 76. TEXT G. LIVER SCAN A liver scan involves injecting a slightly radioactive medium that is taken up by the liver. An instrument is passed over the liver that records the amount of material taken up by the liver and forms a composite “picture” of the liver. The physician may be able to determine tumors, masses, and abnormal size and patterns of blood vessel. The procedure takes a short time.  76
- 77. TEXT H. ULTRASONOGRAPHY The use of high-frequency sound waves through the abdomen allows the physician to view soft- tissue structures. The sound waves reflect varying images based on the density of the soft tissues in the abdomen. The patient is asked not to take anything by mouth after midnight on the day of the examination.  77
- 78. TEXT H. ULTRASONOGRAPHY A clear gel is applied to the abdomen and to the transducer on the sonograph. The gel improves the conduction of sound waves and thus improves the images obtained. The transducer is placed on the skin and moved over the abdomen while the technician views the sonograph screen and takes periodic pictures. The procedure takes about half an hour and requires no follow- up care.  78
- 79. TEXT I.PERCUTANEOUS LIVER BIOPSY If less invasive tests do not aid in diagnosis of liver disease, a liver biopsy may be done. This may be done to identify cancer, cirrhosis, hepatitis, or other causes of liver disease. The physician generally inserts a needle through the skin and into the liver to withdraw a small sample for examination. This procedure places the patient at risk for bleeding because the liver is highly vascular and because many patients with liver disease have reduced clotting ability. Before the biopsy, ensure that the patient understands the procedure and that a consent has been signed if required by institution policy. You should also ensure that laboratory tests, such as a complete blood cell count and coagulation studies, have been completed and reviewed as ordered. The patient may be ordered nothing by mouth for 6 to 8 hours before the procedure. Baseline vital signs are taken, and a sedative is given if ordered.  79
- 80. TEXT During the procedure the nurse assists the physician to position the patient on his or her back or left side and assists the patient to hold very still while the needle is being introduced. The physician may also ask the patient to exhale and hold his or her breath during the needle insertion. After the biopsy, the patient should remain on bedrest for 24 hours. The patient lies on the right side for the first 2 hours with a small pillow or rolled towel under the biopsy site to provide pressure and prevent bleeding. Vital signs and the site are monitored for signs of bleeding. The patient is advised to avoid coughing or straining. I.PERCUTANEOUS LIVER BIOPSY  80
- 81. TEXT I.PERCUTANEOUS LIVER BIOPSY NURSING INTERVENTIONS Signed consent. Ensure laboratory tests such as CBC, coagulation studies have been ordered and reviewed. NPO for 6–8 hours prior to procedure. Rest several hours after procedure; restricted activity 1 day. Monitor biopsy site pressure dressing for bleeding. Monitor vital signs after procedure. Coughing and straining avoided after the procedure. Medicate for pain.  81
- 83. ENDOSCOPIES  83 Endoscopy uses a tube and a fiberoptic system (endoscope) for observing the inside of a hollow organ or cavity. In addition to viewing the structures, the physician can also remove polyps, take biopsy specimens, or coagulate bleeding sites that are identified. A consent form must be signed for any endoscopic procedure.
- 85. TEXT A. ESOPHAGO GASTRODUODENOSCOPY Visualizes the esophagus ,the stomach and the duodenum. The procedure is explained to the patient. Patients may be asked to sign an operative consent form, and a preoperative checklist may be necessary, depending on institution policy. To prevent aspiration of stomach contents into the lungs if vomiting occurs, the patient is NPO for 8 to 12 hours before the procedure. Sedatives such as diazepam (Valium) or midazolam (Versed) may be given before the procedure to help relax the patient.  85
- 86. TEXT COMPLICATIONS Midesophageal perforation can cause referred substernal or epigastric pain. Blood loss secondary to perforation can lead to hematoma formation, which in turn can result in cyanosis and referred back pain. Distal esophageal perforation may result in shoulder pain, dyspnea, or symptoms similar to those of a perforated ulcer. The patient may have a sore throat for a few days. A. ESOPHAGO GASTRODUODENOSCOPY  86
- 87. TEXT NURSING INTERVENTIONS NPO for 8 hours prior to the examination The patient is given a local anaesthetic gargle or spray. sedation to be given like inj midazolam. Atropine may be administered to reduce secretions. The patient is positioned in the left lateral position After gastroscopy, assessment includes level of consciousness, vital signs, oxygen saturation, pain level, and monitoring for signs of perforation (pain, bleeding, rapidly elevated temperature) A. ESOPHAGO GASTRODUODENOSCOPY  87
- 89. TEXT Biliary Obstruction – suspected or known Pancreatic Obstruction – suspected or known Evaluation of signs/symptoms suggesting pancreatic malignancy Evaluation of idiopathic pancreatitis Evaluation of sphincter of oddi by manometry Stent placement High risk pts with large unremovable common duct stones C. ENDOSCOPIC RETROGRADE CHOLANGIO PANCREATOGRAPHY  89
- 90. TEXT Visualize the liver, gall- bladder, and pancreas. The procedure allows both direct viewing and use of contrast medium. An endoscope is passed through the esophagus to the duodenum, where dye is injected that outlines the pancreatic and bile ducts. The patient is prepared for an ERCP in the same manner as for an EGD, with nothing by mouth after 8 p.m. the night before the examination. The patient is asked about allergies to iodine. Ensure that any ordered laboratory studies, such as a prothrombin time, have been done before the procedure and that the patient has removed dentures. The nurse is alert to patient complaints such as increased right upper quadrant pain, fever, or chills, which may indicate infection. C. ENDOSCOPIC RETROGRADE CHOLANCHOLANGIO PANCREATOGRAPHY  90 C. ENDOSCOPIC RETROGRADE CHOLANGIO PANCREATOGRAPHY
- 91. TEXT NURSING INTERVENTIONS NPO after 8 PM the night before exam. Check prothrombin time prior to procedure. Monitor for pain, fever, chills which could indictate infection. Monitor for onset of pancreatitis. C. ENDOSCOPIC RETROGRADE CHOLANCHOLANGIO PANCREATOGRAPHY  91 C. ENDOSCOPIC RETROGRADE CHOLANGIO PANCREATOGRAPHY
- 92. TEXT Ulcerations punctures lacerations tumors hemorrhoids polyps fissures fistulas abscesses can be detected. D. PROCTOSIGMOIDOSCOPY  92
- 93. ANOSCOPY  93 An anoscopy is a procedure that uses a small tube called an anoscope to view the lining of your anus and rectum. A related procedure called high resolution anoscopy uses a special magnifying device called a colposcope along with an anoscope to view these areas. fetal position on a table, insert the anoscope, which is lubricated with K-Y Jelly and visualise Indications • cancer • tears in the tissue called anal fissures • hemorrhoids (swollen veins around the anus and/or rectum) • rectal polyps
- 94. TEXT D. PROCTOSIGMOIDOSCOPY examination of the distal sigmoid colon, the rectum, and the anal canal using a rigid or flexible endoscope Malignancies at an early stage can be detected, so an annual examination for patients 40 years old and older is recommended. Proctosigmoidoscopy requires the lower bowel to be cleaned out. The patient usually receives a clear liquid diet 24 hours before the test and a laxative the night before the test. The morning of the procedure a warm tap- water enema or sodium biphosphate (Fleet) enema is given. Bowel preparation may not be ordered for patients with bleeding or severe diarrhea.  94
- 95. TEXT D. PROCTOSIGMOIDOSCOPY Specimens are labeled and sent to the pathology laboratory immediately for examination. After the procedure, the patient is allowed to rest for a few minutes in the supine position to avoid orthostatic hypotension when standing. Pain and flatus may occur from instilled air. The patient is observed for signs of perforation such as bleeding, pain, and fever.  95
- 96. TEXT D. PROCTOSIGMOIDOSCOPY Nursing interventions These examinations require only limited bowel preparation, including a warm tap water enema or Fleet’s enema until returns are clear. Dietary restrictions are not necessary, and sedations not usually not required. During the procedure the nurse  96
- 97. TEXT E. COLONOSCOPY INDICATIONS Colonoscopy provides visualization of the lining of the large intestine to identify abnormalities through a flexible endoscope, which is inserted rectally. A biopsy specimen may be obtained or polyps be removed during the colonoscopy. The patient receives a liquid diet 24 hours before the test and is NPO after midnight before the procedure. A bowel preparation solution such as GoLYTELY is given the night before the procedure. Drinking this solution can be unpleasant for the patient.  97
- 98. TEXT E. COLONOSCOPY. The patient is encouraged to relax and take slow deep breaths through the nose and out the mouth. Vital signs are monitored throughout the procedure to watch for a vasovagal response, which can lead to hypotension and bradycardia. After the procedure, the patient is monitored until stable. Complications such as hemorrhage or severe pain are reported. When giving the patient discharge instructions, explain that flatus and cramping will occur for several hours after the test, that blood may be present in the stool if a biopsy specimen was taken, and to report problems to the physician.  98
- 99. TEXT E. COLONOSCOPY. Nursing interventions Adequate colon cleansing provides optimal visualization and decreases the time needed for procedure. The physician may prescribe a laxative two nights prior the examination and enema until the return is clear the morning of the test. The patient maintains a clear liquid diet starting at noon the day before the procedure. A sodium phosphate tablet can be used for colon cleansing prior to colonoscopy. Informed consent is obtained by the practitioner before the patient is sedated. Before the examination, an opoid analgesic agent or sedative (eg.,midazolam) is administered to provide moderate sedation and relieve anxiety during the procedure.  99
- 100. TEXT F.ENDOSCOPIC ULTRASONOGRAPHY Endoscopic ultrasonography is performed through the endoscope using sound waves. Tumors can be detected in various GI structures and organs. Preprocedure and postprocedure care are similar to those for endoscopic care. During the test the patient must lie still while a transducer with gel is moved back and forth over the abdomen to produce images.  100
- 101. TEXT F.ENDOSCOPIC ULTRASONOGRAPHY Nursing interventions The patient is instructed to fast for 8 to 12 hours before ultrasound testing to decrease the amount of gas in the bowel. If gallbladder studies are being performed, the patient should eat fat free meal evening before the test. If barium studies are to be performed, they should be scheduled after USG. Otherwise barium could interfere with the transmission of sound waves. Patient who receive moderate sedations are observed for about 1 hour to assess for level of consciousness, orientation and ability to ambulate.  101
- 102. TEXT G. SMALL BOWEL STUDIES There are several methods available for visualization of the small intestine, including capsule endoscopy and double balloon endoscopy Capsule endoscopy allows the non invasive visualization of the entire small intestine, particularly useful in the evaluation of obscure GI bleeding. The technique consists of the patient swallowing a capsule embedded with a wireless miniature camera, a light source, and an image transmission system. Images are transmitted from the end of the capsule to a recording device worn on a belt  102
- 103. TEXT G. SMALL BOWEL STUDIES The capsule is the size of a large vitamin pill (26mm long, 11mm wide, 3.7g in weight). It is propelled through the intestine by peristalsis. This diagnostic procedure is limited by its inability to allow for obtaining tissue samples for histology and for endoscopic therapy. Double balloon enteroscopy, also known as push and pull enteroscopy, has made it possible to visualize the mucosa of the entire small bowel as well as carry out diagnostic and therapeutic internventions The endoscope is advanced using a push and pull technique that involves alternately inflating and deflating the balloons, causes telescoping of the small intestine on to the overtube  103
- 104. TEXT H.ENDOSCOPY THROUGH AN OSTOMY Endoscopy through an ostomy stoma is useful for visualizing a segment of the small or large intestine and may be indicated to evaluate the anastamosis for recurrent disease, or to visualize and treat bleeding in a segment of the bowel.  104
- 106. TEXT A. GASTRIC ANALYSIS To determine the cause of recurrent peptic ulcer disease: To determine the cause of raised fasting serum gastrin level: To support the diagnosis of pernicious anemia (PA) To distinguish between benign and malignant ulcer To measure the amount of acid secreted in a patient with symptoms of peptic ulcer dyspepsia but normal X-ray findings To decide the type of surgery to be performed in a patient with peptic ulcer  106
- 107. TEXT A. GASTRIC ANALYSIS The patient is NPO after midnight the night before the test. For the procedure, a nasogastric (NG) tube is inserted and the contents of the stomach are suctioned out through the tube using a syringe. The NG tube is connected to wall suction, and stomach contents are collected every 15 minutes for 1 hour. The specimens are labeled according to the time they were collected and the order in which they were obtained. The gastric acid is tested for pH using indicator paper or a pH meter. The amount of gastric acid is also measured. Too much hydrochloric acid may indicate a peptic ulcer; too little could be a sign of cancer or pernicious anemia. The gastric acid stimulation test measures the amount of gastric acid for 1 hour after subcutaneous injection of a histamine drug.  107
- 108. TEXT B. GASTRIC MANOMETRY.  108 This test measures electrical and muscular activity in the stomach. The healthcare provider passes a thin tube down the patient's throat into the stomach. This tube contains a wire that takes measurements of the electrical and muscular activity of the stomach as it digests foods and liquids. This helps show how the stomach is working, and if there is any delay in digestion. Evaluation of noncardiac chest pain or esophageal symptoms not diagnosed by endoscopy
- 109. TEXT C. ESOPHAGEAL MANOMETRY. This test helps determine the strength of the muscles in the esophagus. It is useful in evaluating gastroesophageal reflux and swallowing abnormalities. A small tube is guided into the nostril, then passed into the throat, and finally into the esophagus. The pressure the esophageal muscles produce at rest is then measured. ‣ Diffuse esophageal spasm. This rare swallowing problem is characterized by multiple, forceful, poorly coordinated muscle contractions of your esophagus. ‣ Achalasia. This uncommon condition occurs when your lower esophageal sphincter muscle doesn't relax properly to let food enter your stomach. ‣ Scleroderma. In many people with this rare progressive disease, the muscles in the lower esophagus stop moving, leading to severe gastroesophageal re fl ux  109
- 110. TEXT D. ANORECTAL MANOMETRY. This test helps determine the strength of the muscles in the rectum and anus. Anorectal manometry is helpful in evaluating anorectal malformations and Hirschsprung disease, among other problems. A small tube is placed into the rectum to measure the pressures exerted by the sphincter muscles that ring the canal. Anal incontinence Distal constipation Preoperative evaluation before sphincteroplasty or surgical rectocele repair  110
- 111. TEXT E. LAPAROSCOPY Mass or tumor Fluid in the abdominal cavity Liver disease Degree to which a particular cancer has progressed This test uses a long, thin tube with a tiny camera and a light on the end (laparoscope). It is put into a small cut (incision) in the belly (abdomen). It can check the contents of the abdomen and remove tissue samples.  111
- 112. TEXT F.HEPATOBILIARY SCINTIGRAPHY Gallbladder inflammation (cholecystitis) Bile duct obstruction Congenital abnormalities in the bile ducts, such as biliary atresia Postoperative complications, such as bile leaks and fistulas Assessment of liver transplantThis is a nuclear medicine imaging test. It is used to view the liver, bile ducts, gallbladder, and upper part of the small intestine. This may also be called a HIDA or PIPIDA scan. This depends on which nuclear isotope is used.  112
- 113. TEXT G. MAGNETIC RESONANCE This is a type of MRI. It uses radio waves and magnets to take pictures of the bile ducts and organs.  113
- 114. TEXT H. PERCUTANEOUS TRANSHEPATIC CHOLANGIOGRAPHY A needle is put through the skin and into the liver. A contrast dye is injected through the needle. This lets the bile duct be seen on an X-ray.  114
- 115. TEXT I. POSITRON EMISSION TOMOGRAPHY (PET SCAN) PET scans produce images of then body by detecting the radiation emitted from radioactive substances. The radioactive substances are injected in to the body IV and are usually tagged with a radioactive atom such as carbon11, flurine18, oxygen 13. The atoms decay quickly, do not harm the body, have lower radiation levels than a typical x ray or CT scan, and are eliminated through urine or faeces.  115
- 116. TEXT J. DNA TESTING Preclinical diagnosis, and prenatal diagnosis to risk for certain GI disorders (e.g., gastric cancer, lactose deficiency, inflammatory bowel disease, colon cancer. DNA testing allows clinicians to prevent (or minimize) disease by intervening before its onset and to improve therapy. Counselling to learn about the disease and options for preventing and treating the disease, receive support in coping with the situation.  116
- 117. TEXT SUMMARY AND CONCLUSION  117 In order to reach a diagnosis for digestive disorders, a thorough and accurate medical history will be taken by your physician, noting the symptoms you have experienced and any other pertinent information. A physical examination is also done to help assess the problem more completely.There is virtually no risk with the upper and lower GI tests, unless they are repeated several times within a few months' time, when radiation then becomes a risk. Although radiation exposure is minimal, it is greater than for standard still X-rays. Fluoroscopic gastrointestinal examinations are performed by registered and licensed technologists and board-certified radiologists who carefully limit the X-ray to the specific area to be diagnosed so that surrounding parts of the body are not exposed. A lead apron may be worn during the procedure to protect the parts of the body that are not being studied.
- 118. TEXT RESEARCH  118 How can gastro-intestinal tuberculosis diagnosis be improved? A prospective cohort study Abstract Gastrointestinal tuberculosis (TB) is diagnostically challenging; therefore, many cases are treated presumptively. We aimed to describe features and outcomes of gastrointestinal TB, determine whether a clinical algorithm could distinguish TB from non-TB diagnoses, and calculate accuracy of diagnostic tests. Methods We conducted a prospective cohort study of hospitalized patients in Kota Kinabalu, Malaysia, with suspected gastrointestinal TB. We recorded clinical and laboratory characteristics and outcomes. Tissue samples were submitted for histology, microscopy, culture and GeneXpert MTB/RIF®. Patients were followed for up to 2 years. Conclusions The prospective design provides important insights for clinicians managing gastrointestinal TB. We recommend wider implementation of high-performing diagnostic tests such as GeneXpert® on extra-pulmonary samples. Gastrointestinal TB remains diagnostically challenging. An algorithm developed to classify patients presenting with suspected gastrointestinal TB cases was specific but insensitive. Testing of such algorithms in larger populations of patients with suspected gastrointestinal TB will reveal whether a composite clinical score could help categorize patients while awaiting, or in the absence of, further diagnostic information. Wider implementation of existing high-performing diagnostic tests such as GeneXpert® on extra-pulmonary samples, and ongoing investment in new diagnostics development, is needed. We recommend increased access to and uptake of GeneXpert® on gastrointestinal samples in suspected TB cases.
- 119. TEXT BIBLIOGRAPHY  119 Brunner & suddarth’s, Medical-Surgical nursing,(2015) 10th edition, Page 978-990 Joyce.M.Black, Medical-Surgical nursing,(2020) 6th edition 560-590 Williams.S. Linda,Understanding Medical Surgical Nursing, 3rd edition(2007), page 678-690 Taylor Carol, Fundamentals of nursing(2010), 5th edition Chintamani, Lewis Medical-surgical nursing,( 2011), 2nd edition,CBS Publications Priscilla Lemonne, Medical Surgical Nursing, 2nd edition http://www.jpma.org.pk/full_article_text.php?article_id=6346 https://www.insideradiology.com.au/image-guided-liver-biopsy/ https://badgut.org/information-centre/diagnostic-tests-and-procedures/ https://www.mometrix.com/academy/diagnostic-procedures-of-the-gastrointestinal-system/ https://badgut.org/information-centre/diagnostic-tests-and-procedures/ https://www.urmc.rochester.edu/encyclopedia/content.aspx? ContentTypeID=85&ContentID=P00364