







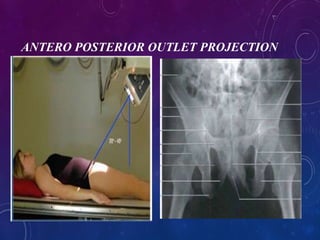






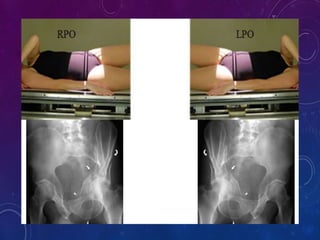





This document provides an overview of various pelvis x-ray projections, including their purposes, patient positioning, technical factors, and image evaluation criteria. It describes the anteroposterior (AP), inlet, outlet, Judet, and flamingo projections. The AP view examines the pelvic ring and bones. The inlet is perpendicular to the pelvic rim. The outlet assesses cephalad/caudal translation following trauma. The Judet views the acetabulum. And the flamingo series evaluates pubic symphysis instability with the patient in neutral, left foot raised, and right foot raised positions. Proper collimation, centering, orientation and other technical parameters are outlined for each view.



































































