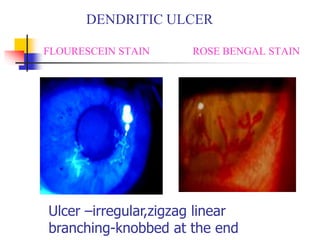
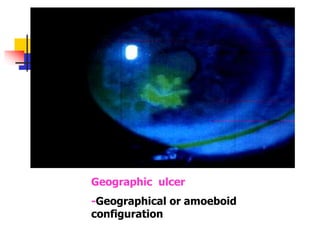
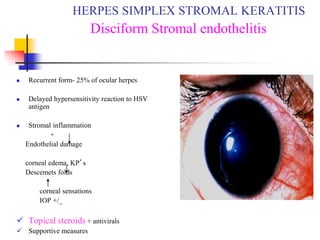
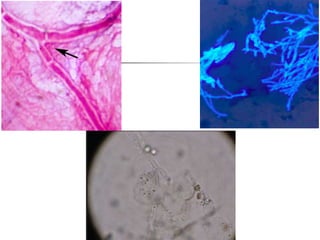
This document discusses diseases of the cornea, including viral keratitis from herpes simplex virus (HSV), herpes zoster virus, and adenovirus. It describes the characteristics, symptoms, signs, and treatment of HSV keratitis, which can present as punctate epithelial keratitis, dendritic ulcers, or geographic ulcers. Recurrent HSV can cause stromal keratitis with inflammation and endothelial damage. Other conditions covered include Acanthamoeba keratitis presenting with severe pain and cysts, fungal keratitis typically caused by Aspergillus, and herpes zoster ophthalmicus affecting the eye in 50% of cases.