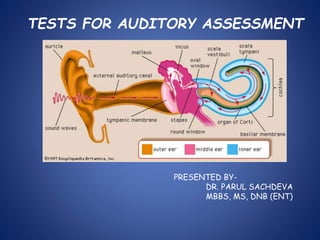
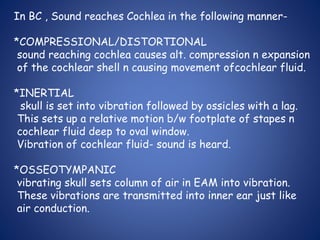
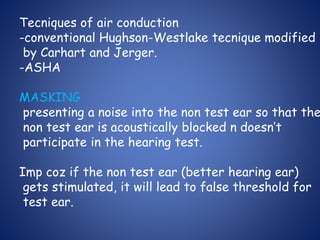
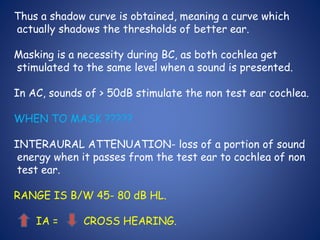
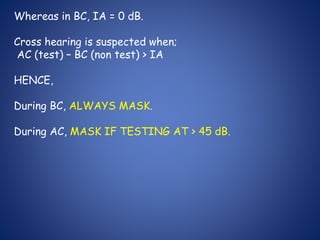
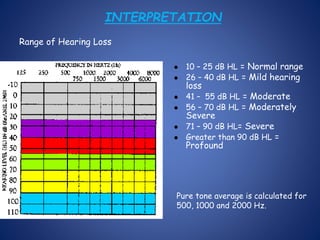
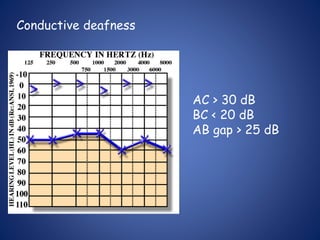
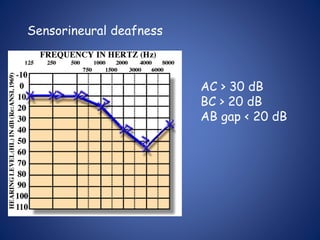
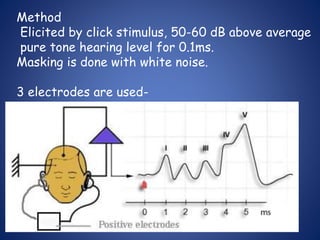
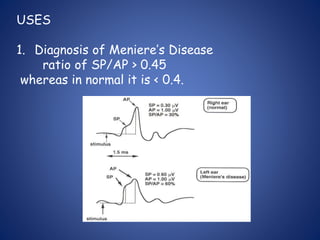
The document presents a comprehensive overview of auditory assessment tests, detailing the types of sound and mechanisms of hearing, as well as various clinical and audiometric tests to evaluate hearing loss. Key tests include tuning fork tests, pure tone audiometry, and impedance audiometry, which help differentiate between conductive and sensorineural hearing loss and determine the degree of dysfunction. It also discusses the interpretation of results, the importance of proper testing conditions, and the use of evoked potentials in evaluating the auditory pathway.























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)

















