






































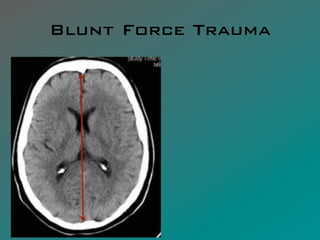








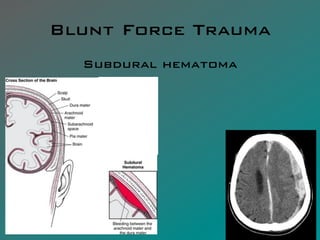























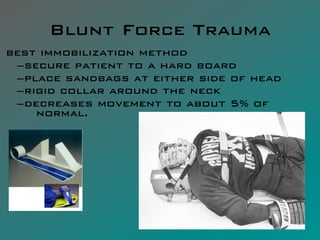










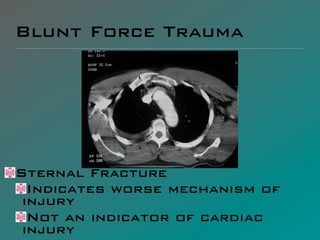














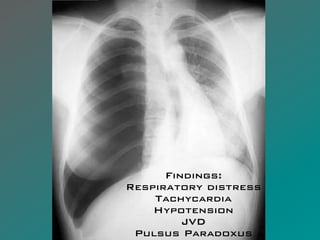


























































The document presents a comprehensive overview of blunt force trauma, detailing types of injuries, anatomical considerations, and specific syndromes associated with such trauma. It discusses injuries related to the head, spine, thorax, and abdomen, including mechanisms of injury and assessment methods for identifying complications. Additionally, it highlights the importance of thorough examination and monitoring for concurrent injuries in emergency settings.