Downloaded 20 times

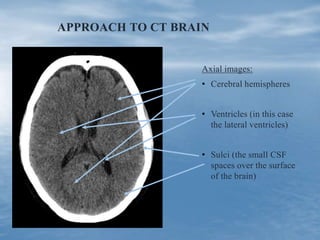
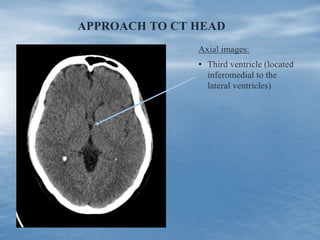
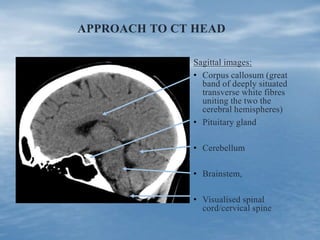
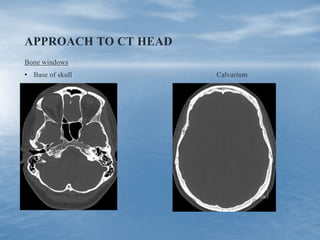
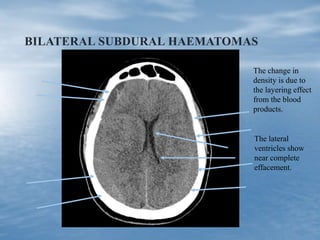
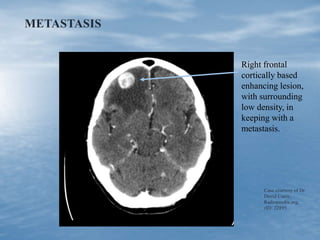
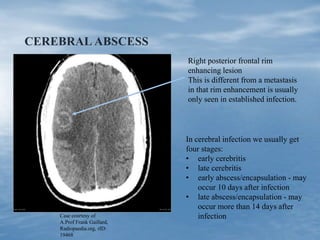
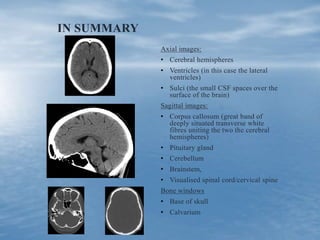

This document outlines an approach for non-radiologists to interpreting CT head scans. It begins with introducing the importance of having a systematic approach similar to clinical exams. The suggested approach examines axial images of the cerebral hemispheres, ventricles, and sulci, as well as sagittal images of the corpus callosum, pituitary gland, cerebellum, brainstem, and spinal cord. Bone windows are also important for examining the base of skull and calvarium. Several case examples are then presented to demonstrate different pathologies including infarcts, traumatic brain injuries, aneurysms, subdural hematomas, metastases, and cerebral abscesses.












































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










