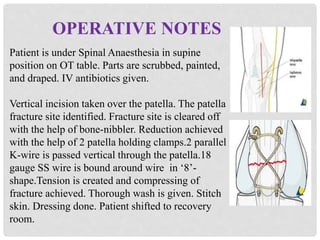
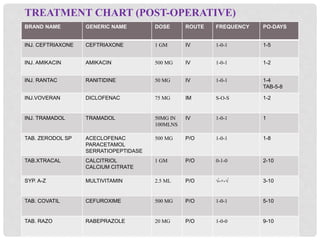
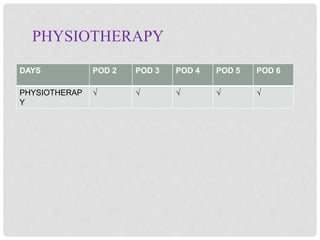
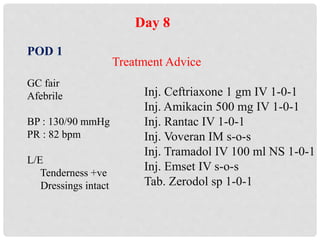
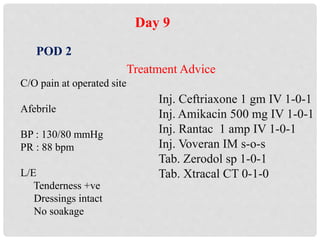
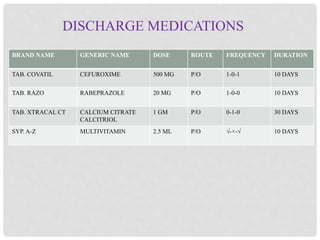
The patient, a 45-year-old female, presented with left patella fracture following a fall. She underwent tension band wiring surgery under spinal anesthesia to repair the fracture. Post-operatively, she was treated with IV and oral antibiotics, analgesics, calcium supplements and physiotherapy. Her pain and swelling gradually reduced and she was discharged on the 10th post-operative day with medications and advice to continue calcium and physiotherapy.