• NAME: LakshmanGaddam
• AGE/GENDER: 77/male
• ADDRESS: Govandi
• DOMINANCE: Right
• OCCUPATION: currently unemployed since 2-3 years ; pre-occupation-Shopkeeper
• DATE OF ADMISSION: 11th
may 25
• DATE OF ASSESSMENT: 12th
April 25
• C/O: B/l excessive knee pain radiating to feet since 3 months
DEMOGRAPHICS:
3.
HOPI:
Patient was apparentlyalright 8 yrs ago
He started experiencing pain in his b/l knees which aggrevated with movement
He took ayurvedic medications which were prescribed by his family dr.
3 years back he experienced excessive pain with varus deformity which had started developing
3 months back due to inability to walk properly and difficulty to perform adls he was brought to MGM
by public transport in sitting position on 11th
may 2025 i.e 1 week back
Since then he is under obs and medications in the male orthopedic ward.
CFS:Patient is oriented to time,place and person ,is able to ambulate with the use of a cane.
4.
PAIN HISTORY
• SIDE: B/L
• SITE : Anterior aspect of the knee radiating towards feet bilaterally.
• TYPE :Dull aching
• ONSET : Gradual
• FREQUENCY : Intermittent
• PROGRESSION : Increased
• DURATION : Since 8 years gradually increased since 3 months chronically.
• A/F: movements at the knee joint and weight bearing
• R/F:Rest
• NRS. ON ACT-5/10
AT REST-0/10
Past Medical History- 2020-
Covid +ve and pneumonitis
Parkinsons disease controlled with
meds since 2020
SURGICAL HISTORY-
2020 bypass surgery for IHD
MEDICATIONS;
1. Atorvastatin-prevents heart attacks
and strokes.reduces triglyceride
and cholesterol levels
2. Levodopa- used for Parkinson
3. Amantrail- for muscle function and
mobility
4. Pacitane- treat symptoms of
parkinsons
5.
PERSONAL HISTORY:
Diet: mixed
Appetite:reduced
Sleep: reduced
Bowel and bladder: regular/continent
Allergies: none
Additions: pre-hospitalization-consumes alcohol and cigratte (1-2) daily
occasional tobacco consumption
SOCIOECOMOMIC HISTORY:
No of people: 1
No of earners: 0
Ration card: saffron
ENVIRONMENTAL HISTORY:
Non-slippery tiles
No stairs
Has duplex house
Transportation available and hospital is nearby
ON OBSERVATION:
• Varusdeformity b/l
• Shinny and scaly skin over shin and feet
• Loss of hair Over distal leg
• Hip laterally rotated
• Edema present at the feet bilaterally
• Swelling present at bilateral knees
On palpation:
• Warmth:present over left lateral side of the knee
• Tenderness: right- grade 1 over medial aspect of the knee
left- grade 2 over medial spect of knee
• Swelling:
Right knee Left knee Difference
73cm 89cm 15cm
• Edema: Grade 1 edema present at b/l feet
L
R
18.
On examination:
• Rangeof motion:
Hip joint left right End feel
Flexion 20-100˚ 10-103˚ Soft tissue appr
Extension 0-20 0-25 firm
Abduction 0-25 0-27 Firm
Knee joint left Right End feel
Flexion 35-100 16-120 empty
extension 100-14 120-8 firm
Ankle joint left Right End feel
Dorsiflexion 0-17 0-10 firm
Plantaflexion 0-40 0-38 firm
left Right
Extensor lag 55 50
Left Right
Hip flexors4 4
abductors 2+ 2+
extensors 2+ 2
Knee flexors 2+ 2+
extensors 4 4
Ankle dorsiflexors 4+ 4
plantaflexors 4+ 4
• MMT
• Tightness assessment: b/l moderate hamstring tightness and
b/l mild TA tightness
27.
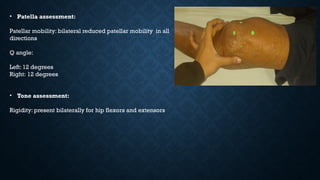
• Patella assessment:
Patellarmobility: bilateral reduced patellar mobility in all
directions
Q angle:
Left: 12 degrees
Right: 12 degrees
• Tone assessment:
Rigidity: present bilaterally for hip flexors and extensors
28.
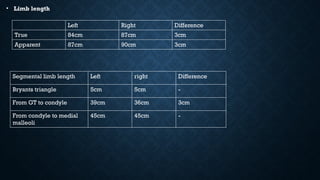
• Limb length
Segmentallimb length Left right Difference
Bryants triangle 5cm 5cm -
From GT to condyle 39cm 36cm 3cm
From condyle to medial
malleoli
45cm 45cm -
Left Right Difference
True 84cm 87cm 3cm
Apparent 87cm 90cm 3cm
MANAGEMENT
Short-Term Goals (0–6weeks):
• Reduce pain and inflammation
• Improve joint mobility and flexibility
• Maintain muscle strength
• Prevent further joint degeneration
Long-Term Goals (6 weeks onward):
• Improve functional independence (gait, ADLs)
• Enhance quadriceps and gluteal muscle strength
• Reduce fall risk
• Improve quality of life and participation in activities
34.
1. Patient Education& Lifestyle Modification
Joint protection techniques
• Use of assistive devices (cane/walker) to reduce load on knees
• Weight management advice
• Ergonomics: Chair height, avoiding squatting or sitting cross-legged
• Use of proper body mechanics
• Pacing and resting
2. Pain Management
• Thermotherapy: Hot packs before exercise
• Cryotherapy: For post-exercise soreness
• TENS or IFT for pain relief
• Topical analgesics as prescribed
35.
3. EXERCISE THERAPY
PhaseI (Weeks 1–2): Focus
on Pain Relief and Mobility
• Mini squats with support
• Sit-to-stand training
• Step-ups with low height
• Proprioception exercises (using
wobble board or foam pad)
• Gait training with/without
assistive device
• Aquatic Therapy
(Hydrokinesiotherapy):Utilizes
water's properties to reduce
joint stress and enhance
mobility.
• Isometric Quadriceps
exercises
• Ankle pumps (to prevent
DVT)
• Heel slides for ROM
• Straight leg raises (SLR)
Phase II (Weeks 3–6):
Muscle Strengthening
• Closed kinetic chain
exercises (within pain-free
range)
• Terminal knee extension with
theraband
• Wall slides (partial)
• Clamshells to strengthen
gluteus medius
• Hamstring curls
• Note: Emphasize correcting
biomechanics—gluteal and
hip strengthening help reduce
medial joint load.
Phase III (6 weeks
onwards): Functional &
Balance Training
RECENT ADVANCES
1. BloodFlow Restriction (BFR) Training
• Low-load strength training using cuffs
• Shown to improve muscle strength and reduce pain in elderly OA patients
• Article: Centner et al., 2019 – Sports Medicine
39.
• Virtual Reality(VR) Rehabilitation:
• Enhances patient engagement and adherence.
• Improves balance and proprioception.
• Facilitates remote therapy sessions.