
Recommended
More Related Content
What's hot
What's hot (20)
Similar to CHRONIC COLITIS: SIGNS, SYMPTOMS, AND TREATMENT
Similar to CHRONIC COLITIS: SIGNS, SYMPTOMS, AND TREATMENT (20)
Recently uploaded
Recently uploaded (20)
CHRONIC COLITIS: SIGNS, SYMPTOMS, AND TREATMENT
- 2. DEFINITION Colitis is inflammation of your colon, also known as your large intestine. Polietiological disease characterized by inflammatory and degenerative changes in the mucosa and impaired function of the colon. Pathologists use the word chronic to describe any condition that has been going on for a prolonged period of time. For many patients with chronic colitis, inflammation may have been present in the colon for months or even years before a diagnosis is made.
- 3. The colon The colon is divided into sections which include the cecum, ascending colon, transverse colon, descending colon, sigmoid colon, and rectum. The colon absorbs water from the food that we eat and move waste out of the body.
- 5. Classification By localization : • total • segmental (rightsided, cecitis, transversitis , sigmoiditis , Proctosigmoiditis ) Phases of the disease : acute phase ; • phase of partial remission ; • phase of complete remission . Severity : • mild ; • moderate ; • severe . By the nature of functional disorders : • with impaired motor function of the colon ; • without dysfunction ; • with symptoms of intestinal dyspepsia ; • without the effects of intestinal dyspepsia . The morphological features : • catarrhal ; • atrophic ; • mixed .
- 7. Etiology The most common cause of chronic colitis is inflammatory bowel disease (IBD). There are two types of inflammatory bowel disease, ulcerative colitis, and Crohn’s disease. Because both types of IBD can look similar when examined under the microscope, you may not be able to say whether the changes seen in your tissue sample are caused by ulcerative colitis or Crohn’s disease.
- 9. Clinics The clinical picture of chronic colitis is dependent on the etiology , localization process , the degree of morphological and functional changes in the intestine. • abdominal pain – character :aching, pressing, sometimes paroxysmal appearing, aggravating factor- 30-90 minutes after eating, before stool, Localized in different departments , but can be spilled , often radiates to the back , the area of the anus , decreases after a bowel movement or flatus . • When distributing the pathological process in the bowel serosa ( pericolitis ) or lymph nodes ( mesadenitis ) pain is constant monotonous character , not associated with food intake , but can be aggravated by motion, after defecation, from warmer .
- 10. Clinics A violation of stool: At one and the same patient may has unstable stool , constipation alternating with diarrhea. Urging to stool may disturb immediately after meals , at bedtime. Often patients complain of incomplete emptying of the bowel . There are so-called " locking diarrhea " when constipation is replaced once or twice a profuse diarrhea. Flatulence Bloating located mainly in the lower and lateral parts , accompanied by rumbling , a feeling of heaviness In some patients the dyspeptic symptoms (nausea, burping air , bitter taste in the mouth , loss of appetite ) . Patients concerned about poor sleep , weakness, irritability, emotional lability .
- 11. • In the absence of total lesions of the colon, clinical manifestations associated with localization of pathological process . 1. In right-sided colitis or diarrhea cecitis often observed up to 10 times a day, pain in the right part of the abdomen , especially in the iliac region , radiating to the leg, loin . On palpation revealed spasm or extension of the cecum . 2. Transversitis - the defeat of the transverse colon - is characterized by pain , rumbling , feeling of fullness in the middle of the abdomen, appearing immediately after a meal , alternating constipation and diarrhea . With the defeat of the splenic flexure of the colon ( Angulitis ) patient concerned severe pain in the left upper quadrant, radiating to the back and left side of the chest , unstable stool , a loud rumbling in the right upper quadrant . When percussion in the left upper quadrant determined thympanitis , palpation - soreness. 3. Left-sided colitis ( proctitis, sigmoiditis , Proctosigmoiditis ) are the most common . This form is characterized by pain in the left iliac region , rectum , tearing in mesogaster worse after a bowel movement. Possible false desires with flatus and mucus. On palpation the sigmoid colon cut , sore , swollen gases. It can be defined dense stool , giving it a lumpy appearance.
- 12. Diagnosis • The diagnosis of chronic colitis is based on 1. medical history 2. clinical data 3. results coprological and bacteriological examination of feces 4. confirmed by barium enema 5. sigmoidoscopy 6. colonoscopy with biopsy mandatory and morphological study of mucosal biopsies 7. ultrasound of the colon.
- 13. When examining tissue samples from the colon under the microscope, pathologists look for specific microscopic changes before making the diagnosis of chronic colitis. Some of these changes tell your pathologist that the damage has been ongoing for a long period of time. These changes include 1. crypt distortion 2. basal lymphoplasmacytosis 3. and Paneth cell metaplasia. Other changes tell your pathologist that the damage is active and continuing to cause new damage. These changes include 1. Cryptitis 2. crypt abscesses 3. and ulcers.
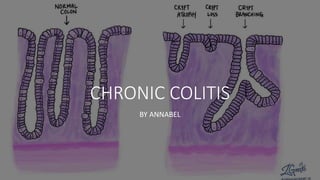
- 14. • Atrophy – Atrophy is a loss of tissue compared to normal. In the colon, atrophy means that the crypts that are seen are smaller than normal, healthy crypts. • Crypt loss – There is a complete loss of crypts in some areas of the mucosa. • Branching – Instead of being long and straight, these crypts split to form multiple branches. Crypt distortion
- 19. • Granulomas are a sign of chronic colitis. It is a clue that the changes seen are caused by Crohn’s disease rather than ulcerative colitis
- 20. Treatment given the state of the patient and the phase of the disease , it can be performed on an outpatient basis or in the hospital. 1. gentle mechanical and chemical diet , split meals 4-6 times a day . 2. Supplied food must be in a shabby , cooked by steaming or broth. 3. Should be excluded from the diet, , milk , salted, smoked and spicy dishes . Patients with severe constipation shown products containing adequate amounts of fiber , dietary fiber , as well as vegetable and fruit juices . 4. Stop alcohol consumption
- 21. pharmacological 1. astringent for diarrhea , enveloping and adsorbing agents : De-nol , smectite (1 pack . 3 times a day ) , bismuth nitrate (1 g three times a day) . 2. Normalization of motor-evacuation function diarrhea contributes metaclopramide ( 0.001 3 times a day ) . Have a similar effect and decoctions of plants containing tannins - fruits dried blueberries, oak bark , sage leaf , stems alder. Flatulence in fees herbs suitable to add the cumin seeds , fennel , chamomile . 3. In the presence of inflammatory changes of the mucous shown antibacterial drugs . Increasingly used sulfa - ftalazol (0.5 to 4 times a day) , nitrofuranovye drugs - furagin , furadonin ( 0.1 , 3 times a day) . Treatment 7-14 days. 4. When expressed pain syndrome prescribe antispasmodics ( drotaverin , Nospanum ) platifillin . 5. With the defect of the rectum have a good effect microclysters - oil ( sea buckthorn, rose) , decoction of chamomile.
- 22. Treatment physiotherapy - electrophoresis with novocaine platifillina , calcium chloride , UHF , ultrasound, Amplipuls , diathermy, warm baths, hot compress . If necessary, in the range of therapeutic interventions include sedatives , psychotherapy , acupuncture . Sanatorium treatment indicated only in remission ( sanatorium " Krynica ", " Riverlands " resorts "Naroch ", " Bobruisk ," " Druskeninkay ", " Essentuki" ).
- 23. Medical and social assessment • During an exacerbation of chronic colitis patients need relief from work. In chronic colitis patient contraindicated moderate trips, daily and night shifts . Limitation of employment may necessitate the establishment of their three disability groups .
- 24. Prevention prevent acute intestinal infections elimination of chronic foci of infection compliance culture and nutrition healthy lifestyle Restriction of the use of alcohol constant physical training and sports strengthening the nervous system.
- 25. The end Thanks for your attention