Downloaded 248 times
![The Spine & Spinal Cord Faisal Majid 4 th year (Endo BSc) MM Education rep [email_address]](https://image.slidesharecdn.com/thespinespinalcord-110312172622-phpapp01/75/The-spine-spinal-cord-1-2048.jpg)
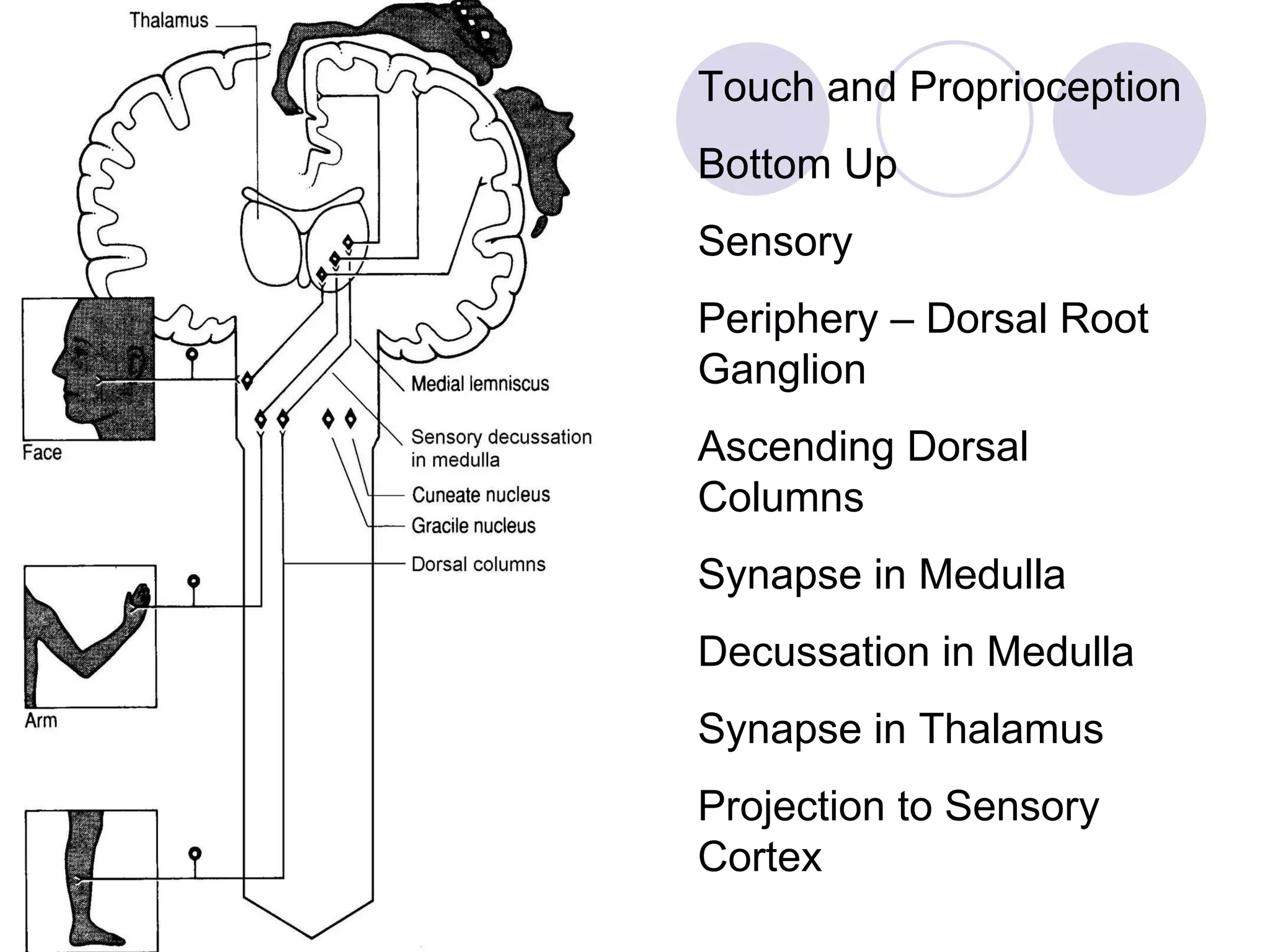
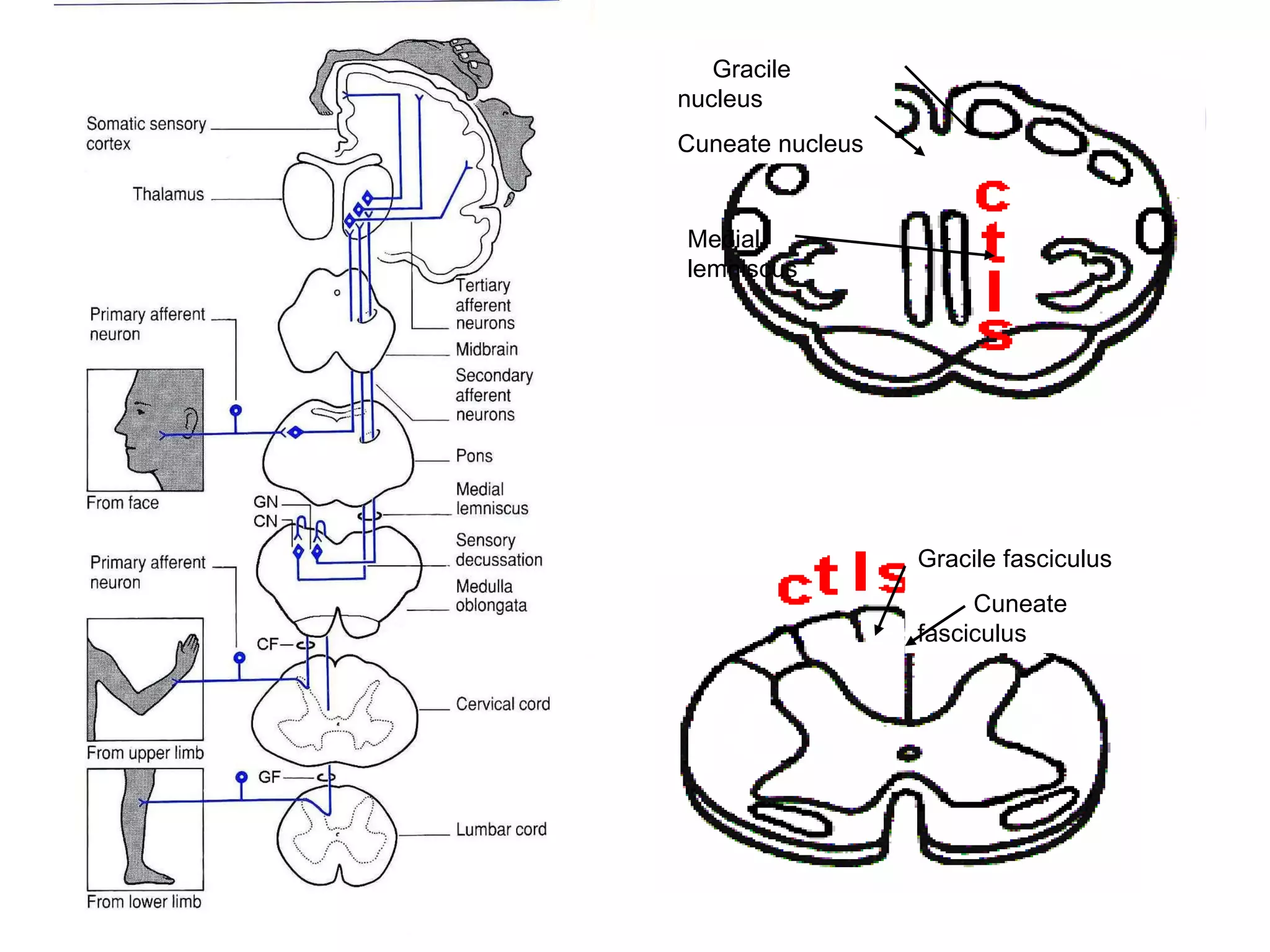
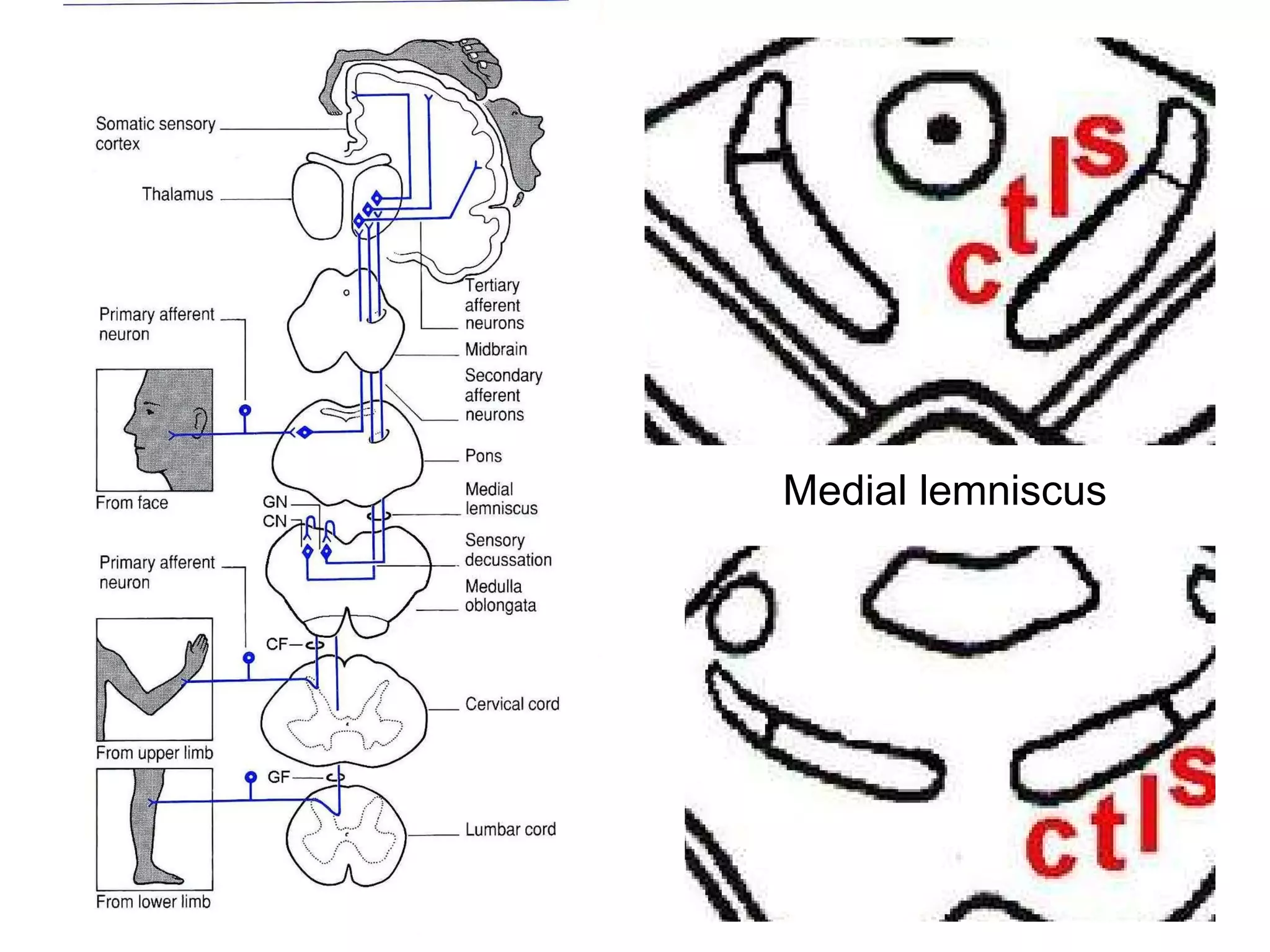
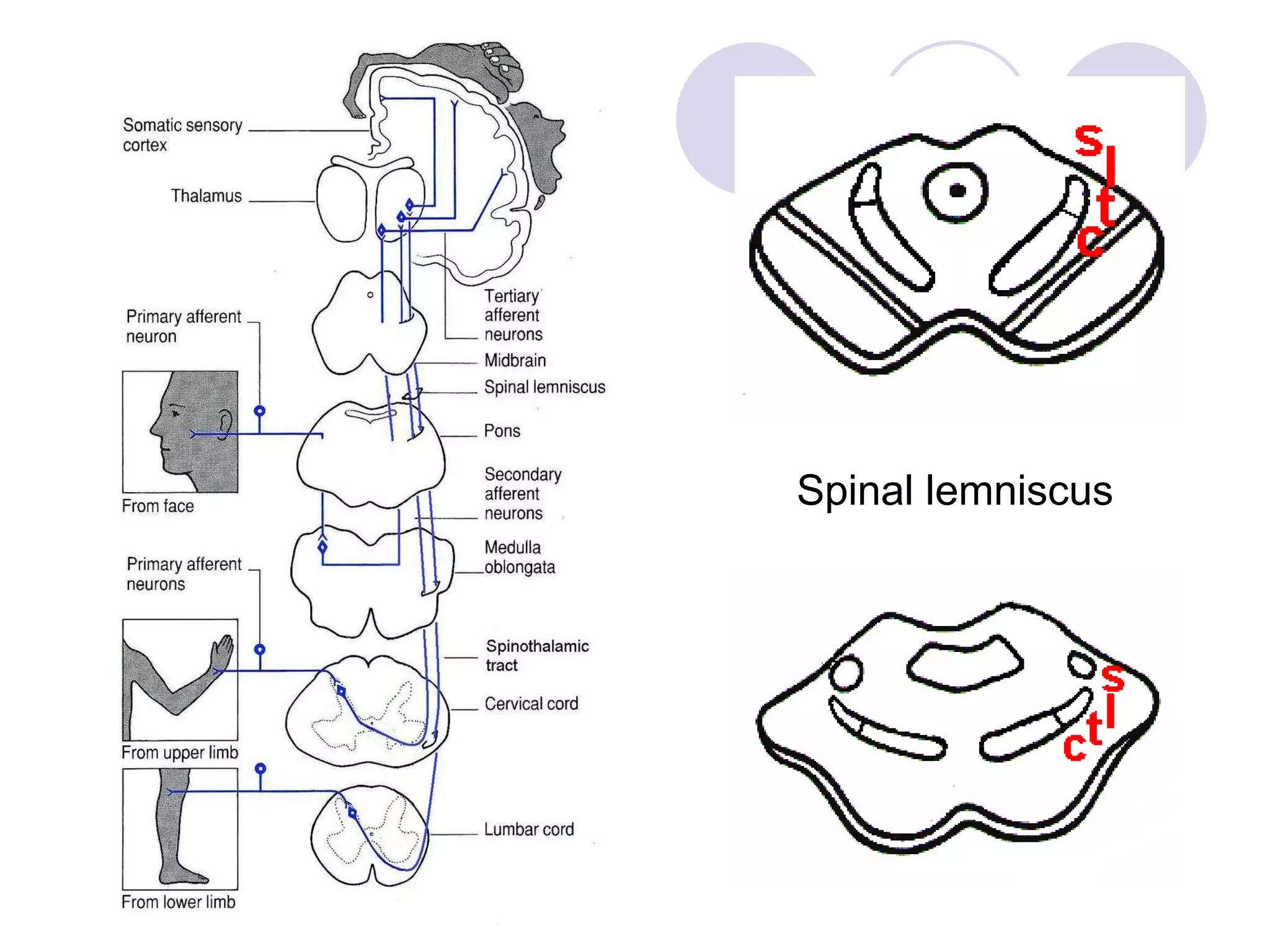
![Central pathway [touch & proprioception] Fasciculus Gracilis (M) Fasciculus Cuneatus (L) Tirgeminal CROSS IN MEDULLA UMN – CONTRALATERAL LMN - IPSILATERAL](https://image.slidesharecdn.com/thespinespinalcord-110312172622-phpapp01/75/The-spine-spinal-cord-30-2048.jpg)
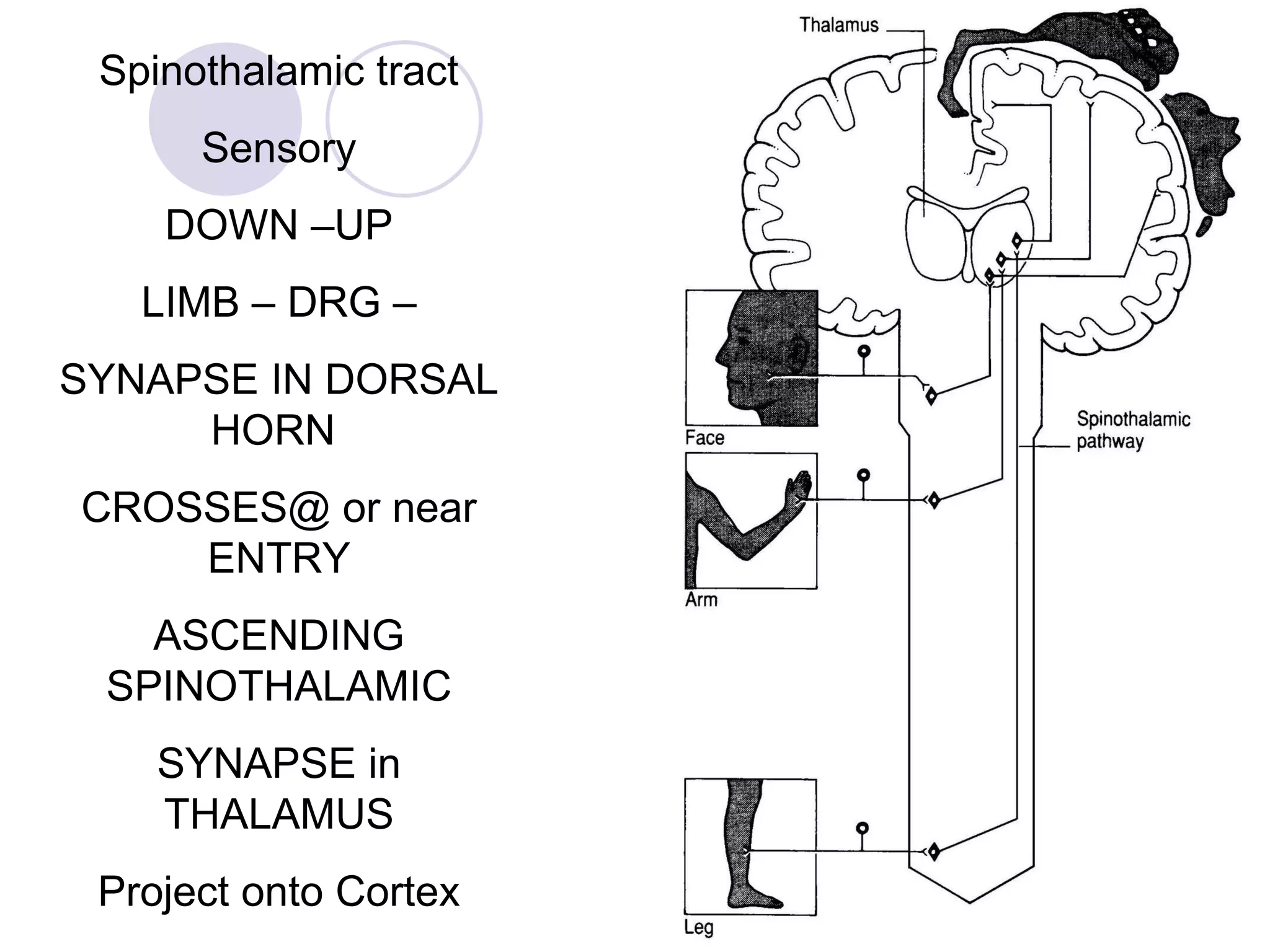
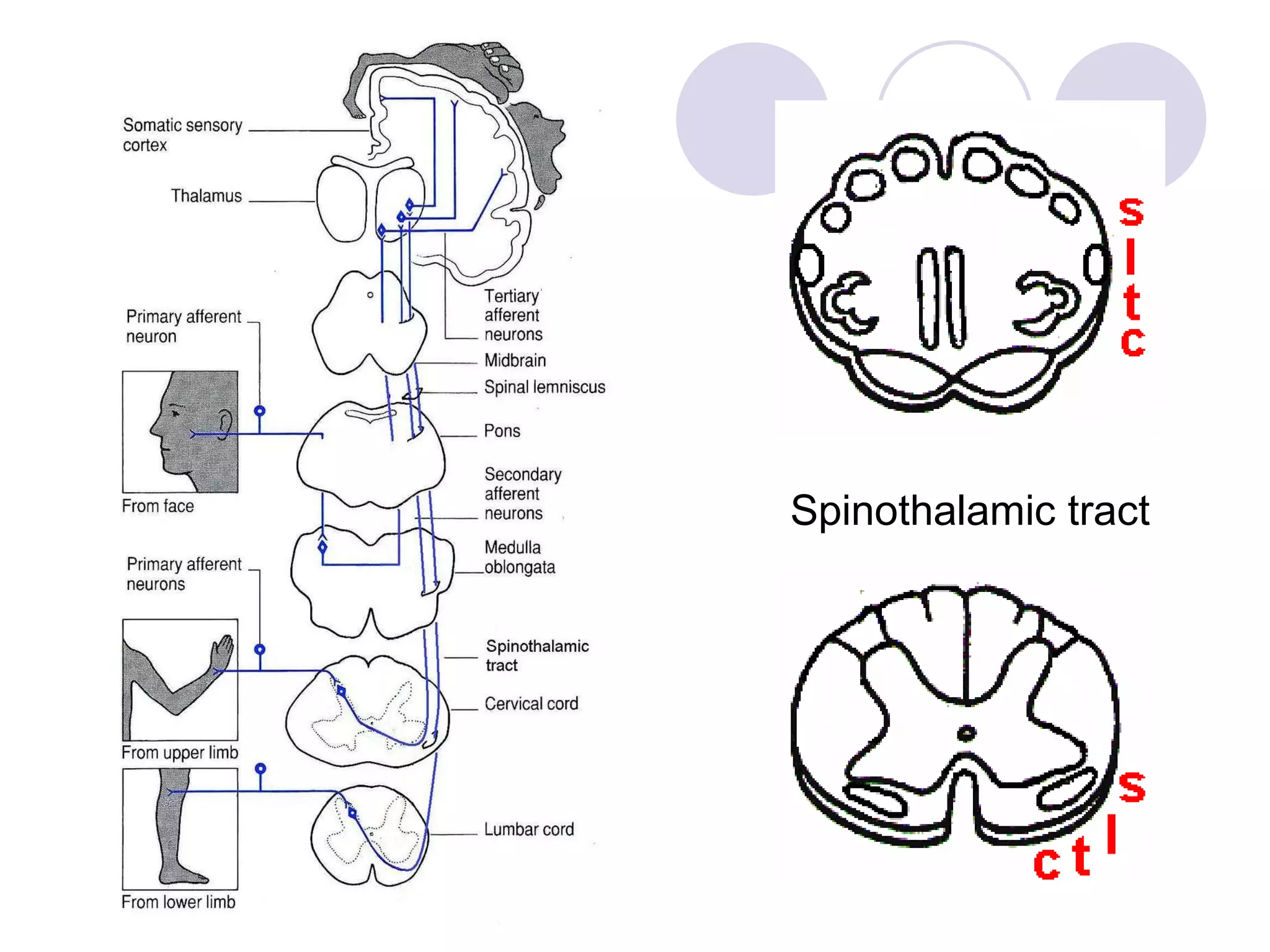
![Central pathway [pain & temperature] SLTC TRIGEMINAL UMN – Contralateral LMN - CONTRALATERAL](https://image.slidesharecdn.com/thespinespinalcord-110312172622-phpapp01/75/The-spine-spinal-cord-34-2048.jpg)



The document discusses anatomy of the spine, including identifying vertebrae and describing their features. It covers the roles of intervertebral discs, ligaments, and muscles in load bearing and spinal movement. Common spinal abnormalities and causes of back pain are outlined. Procedures like lumbar puncture and considerations for spinal injury management are also summarized.
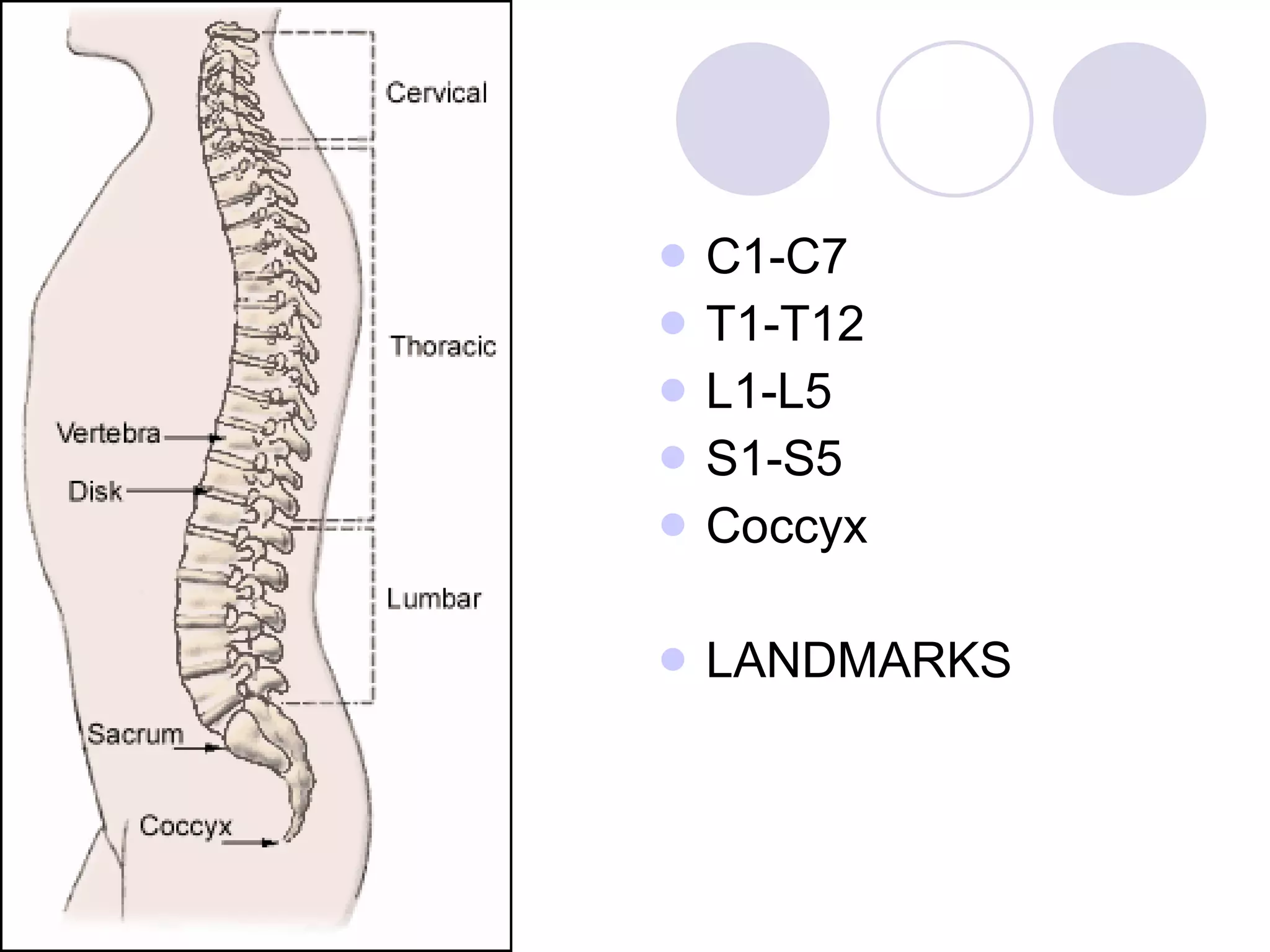
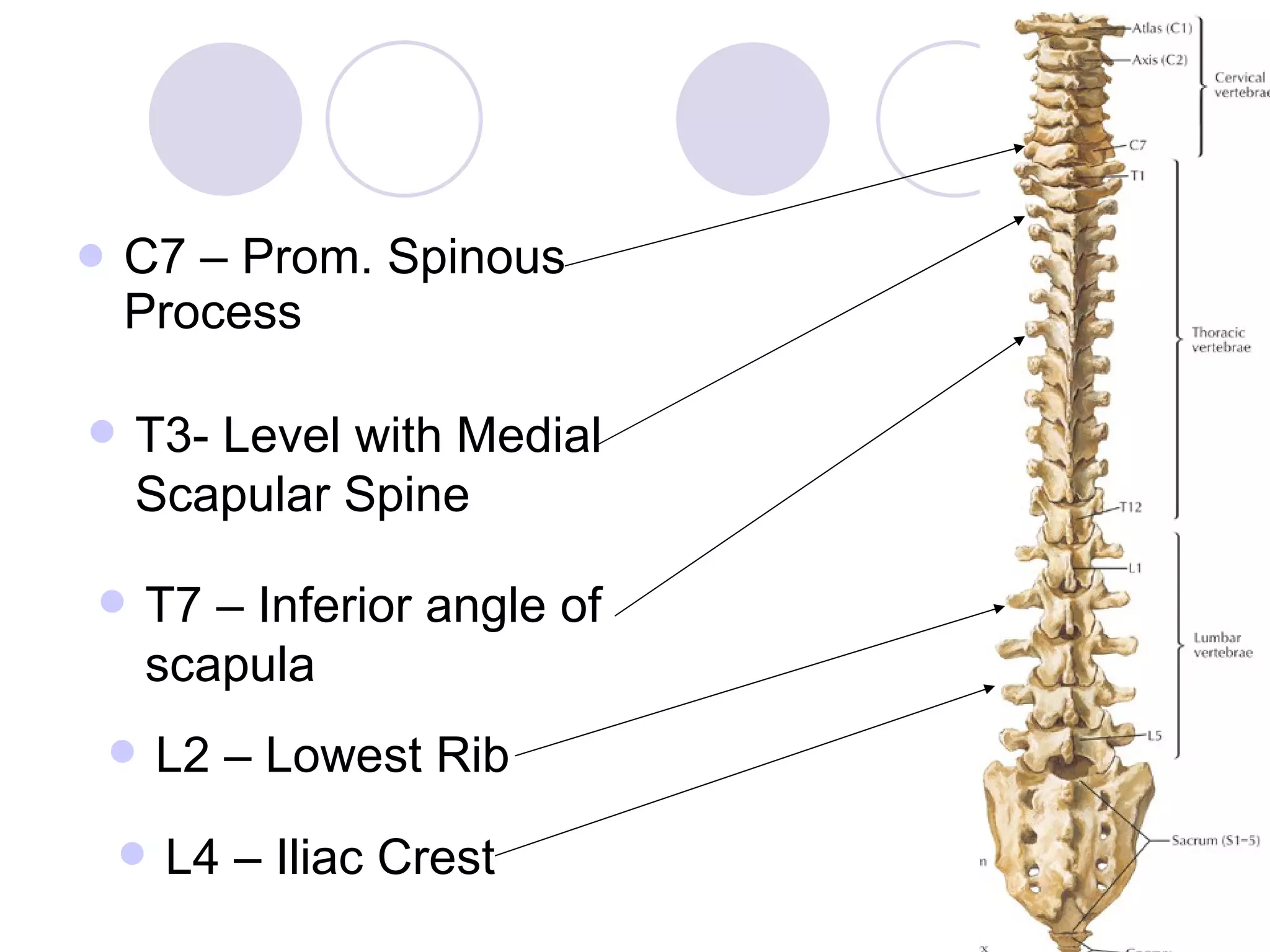
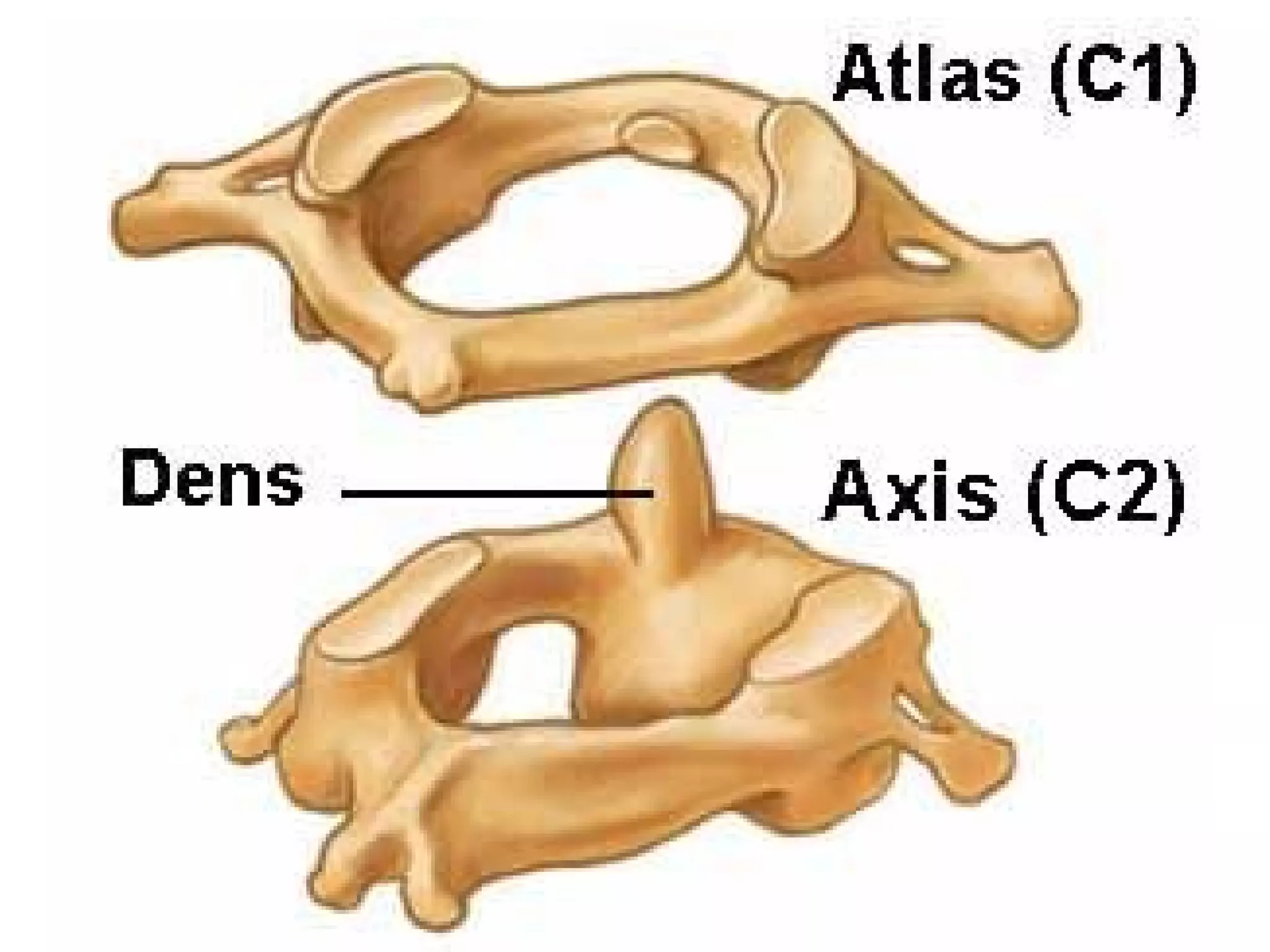
Introduction to spine anatomy and vertebrae types along with their landmarks in cervical, thoracic, and lumbar regions.
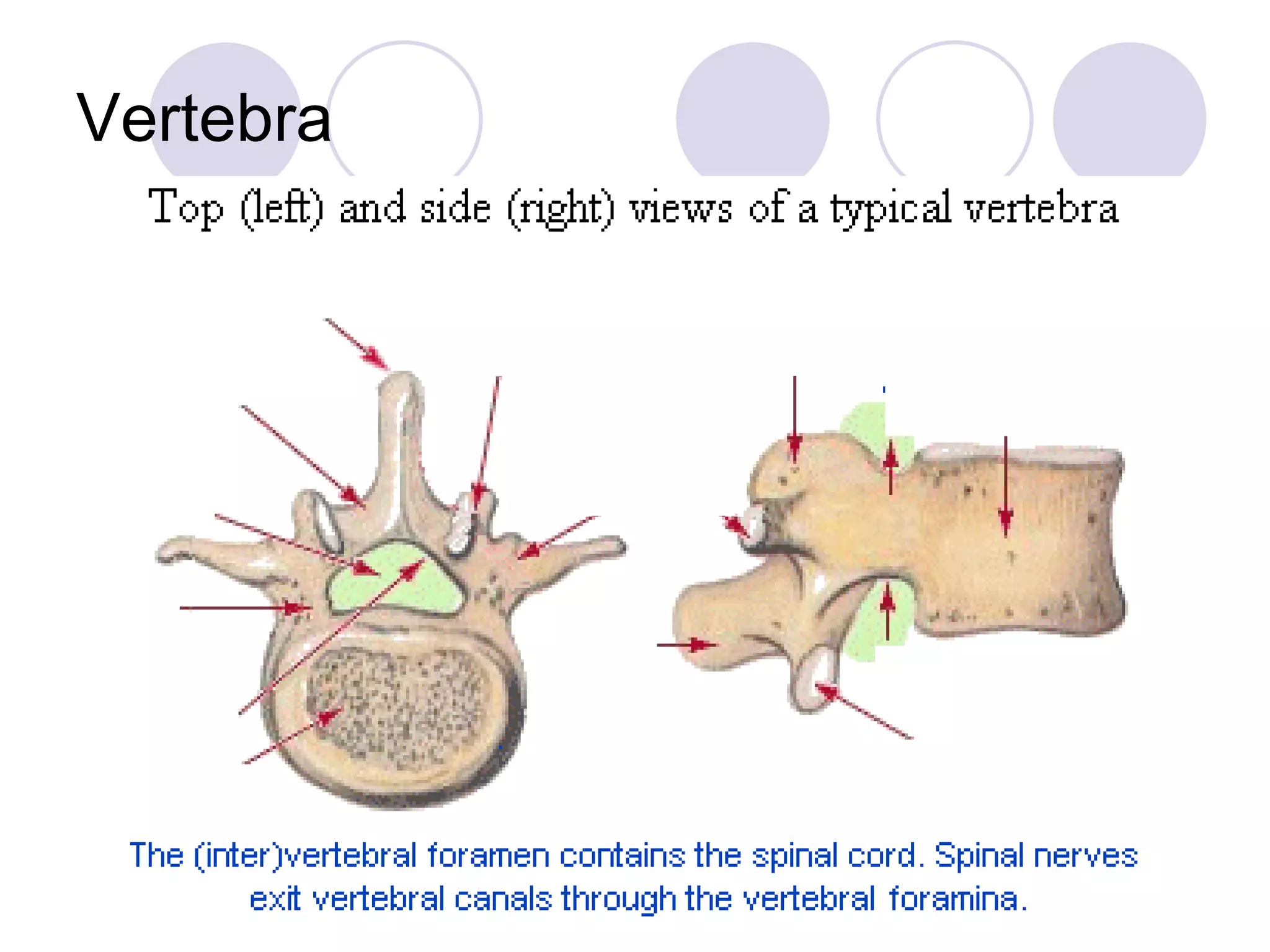
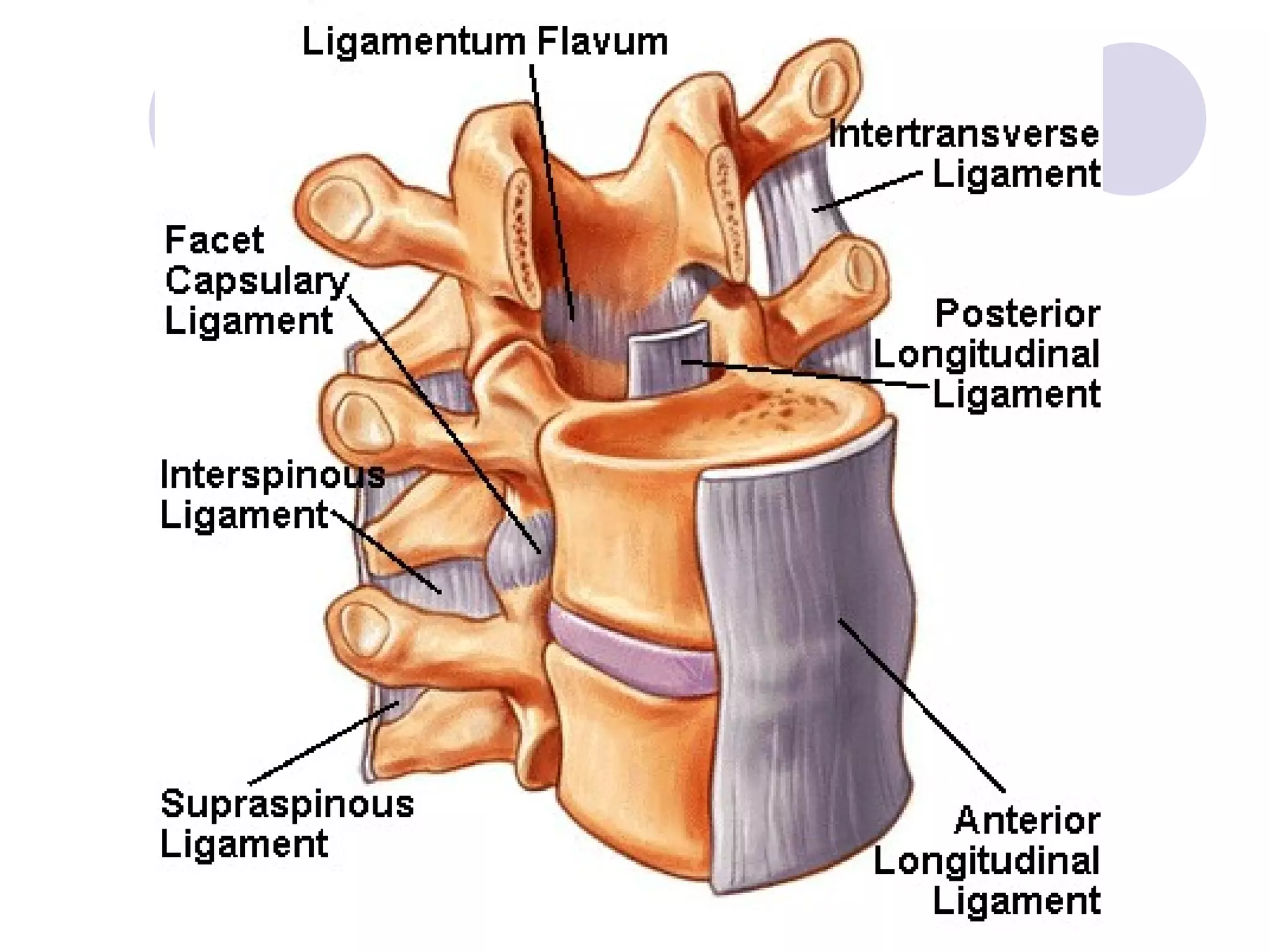
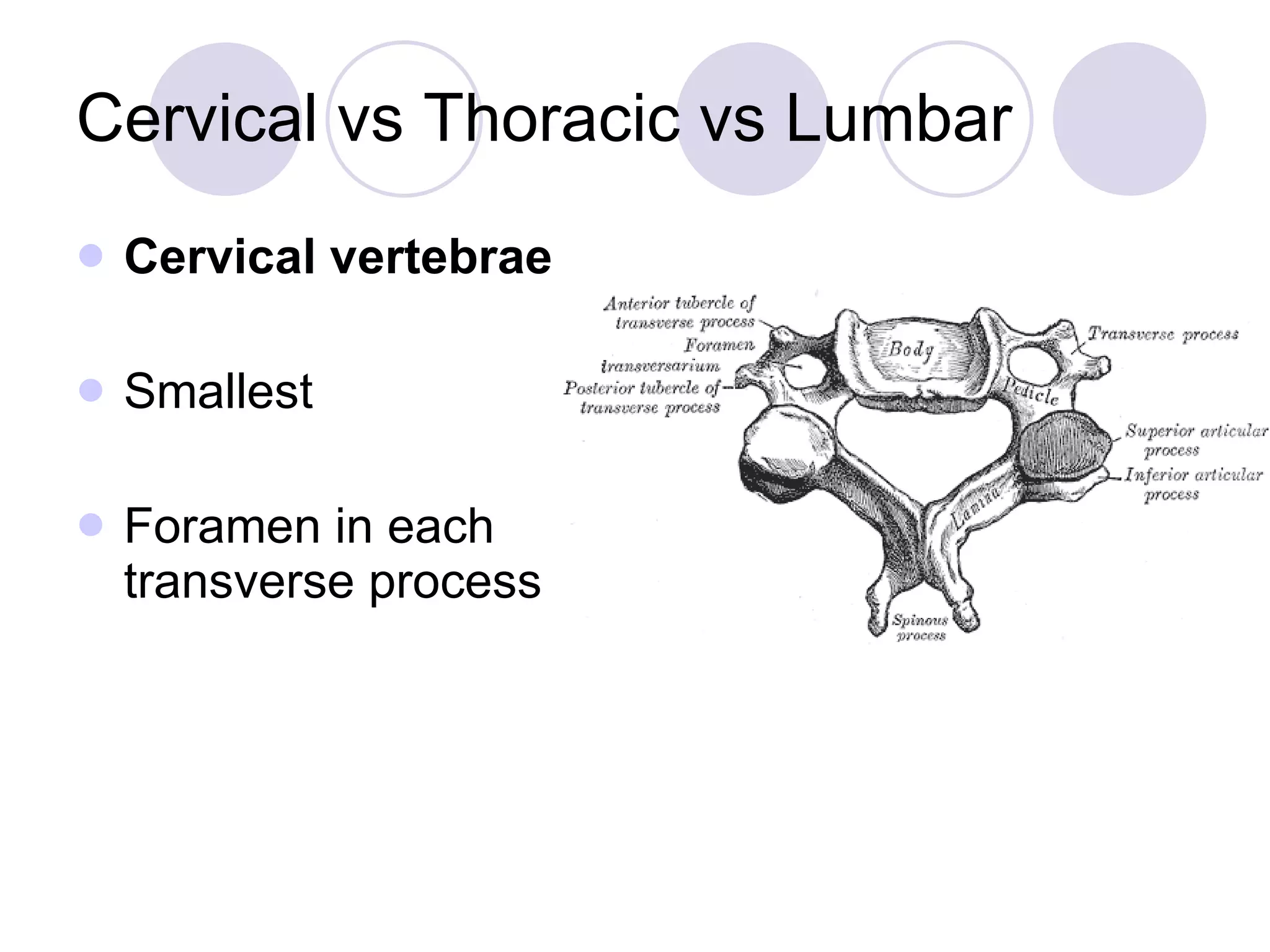
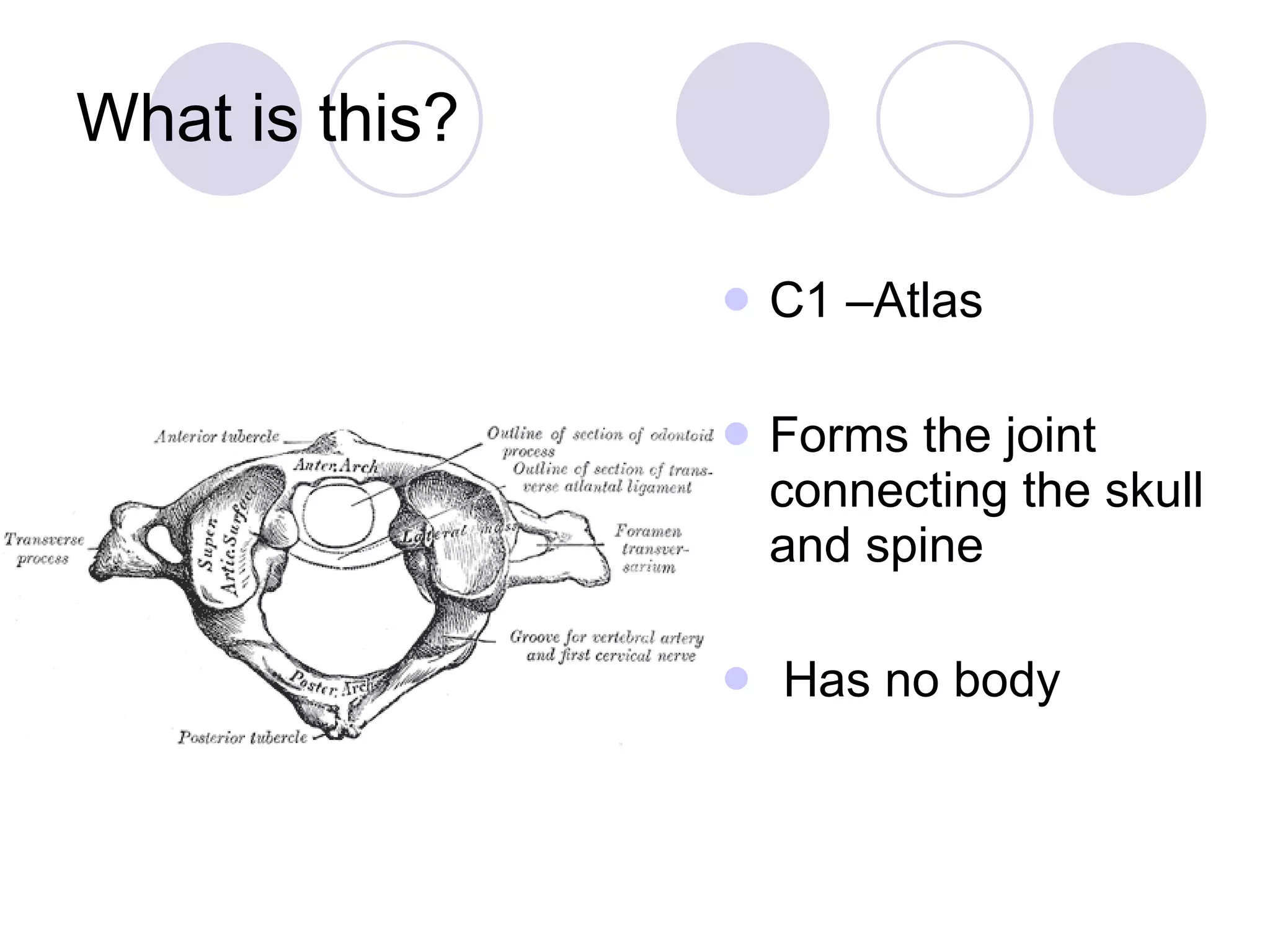
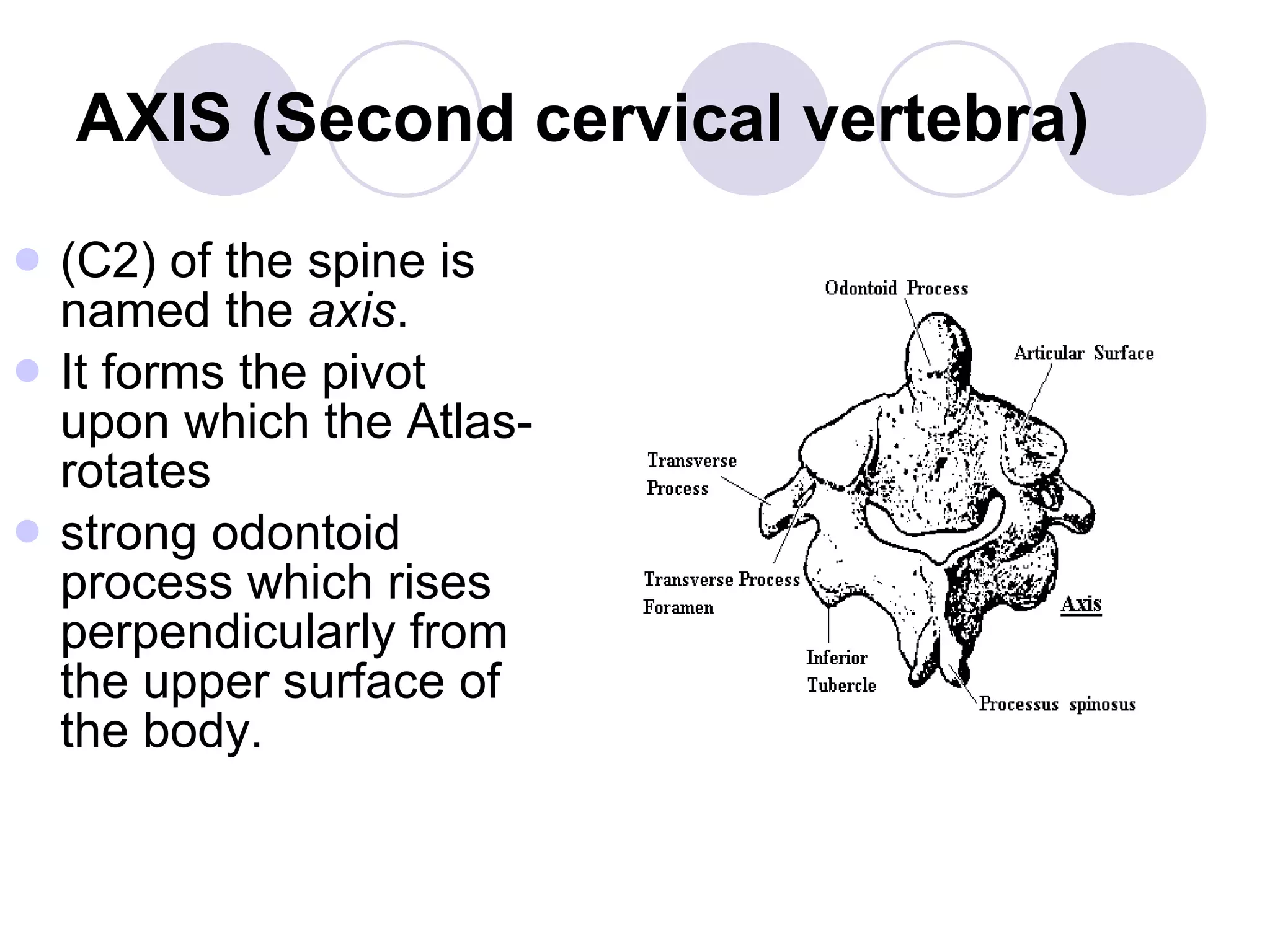
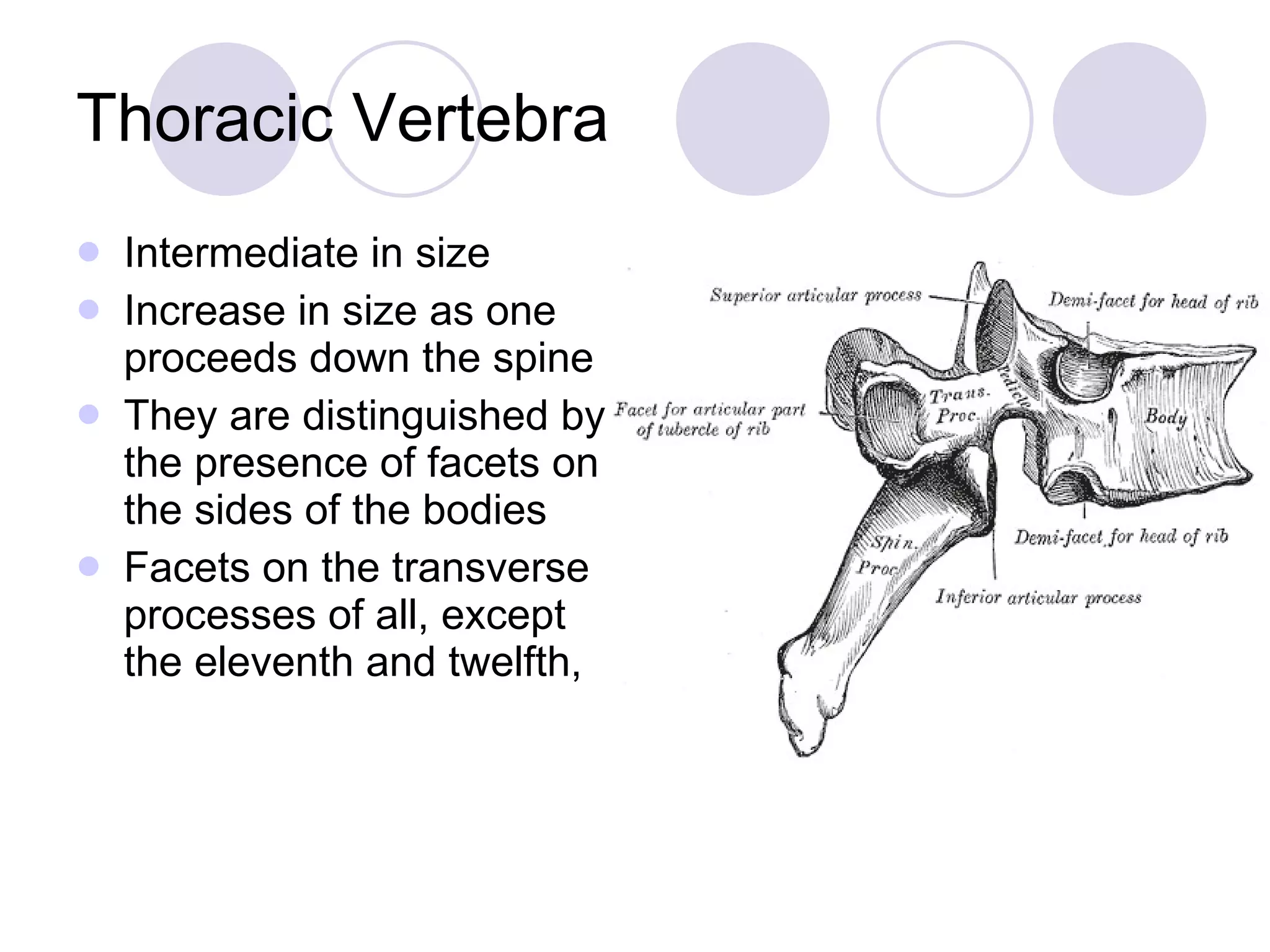
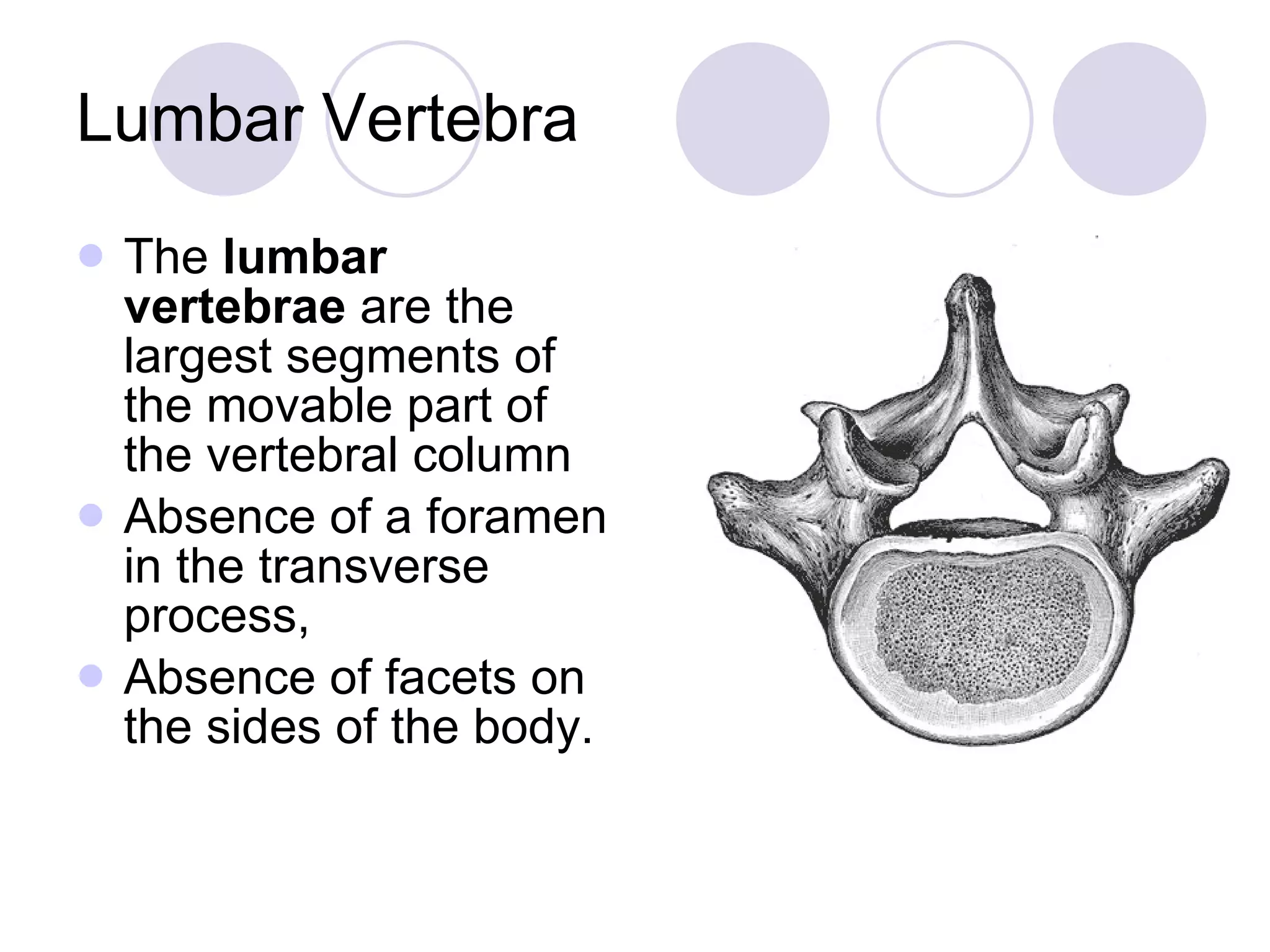
Detailed features distinguishing cervical, thoracic, and lumbar vertebrae, including their structures.
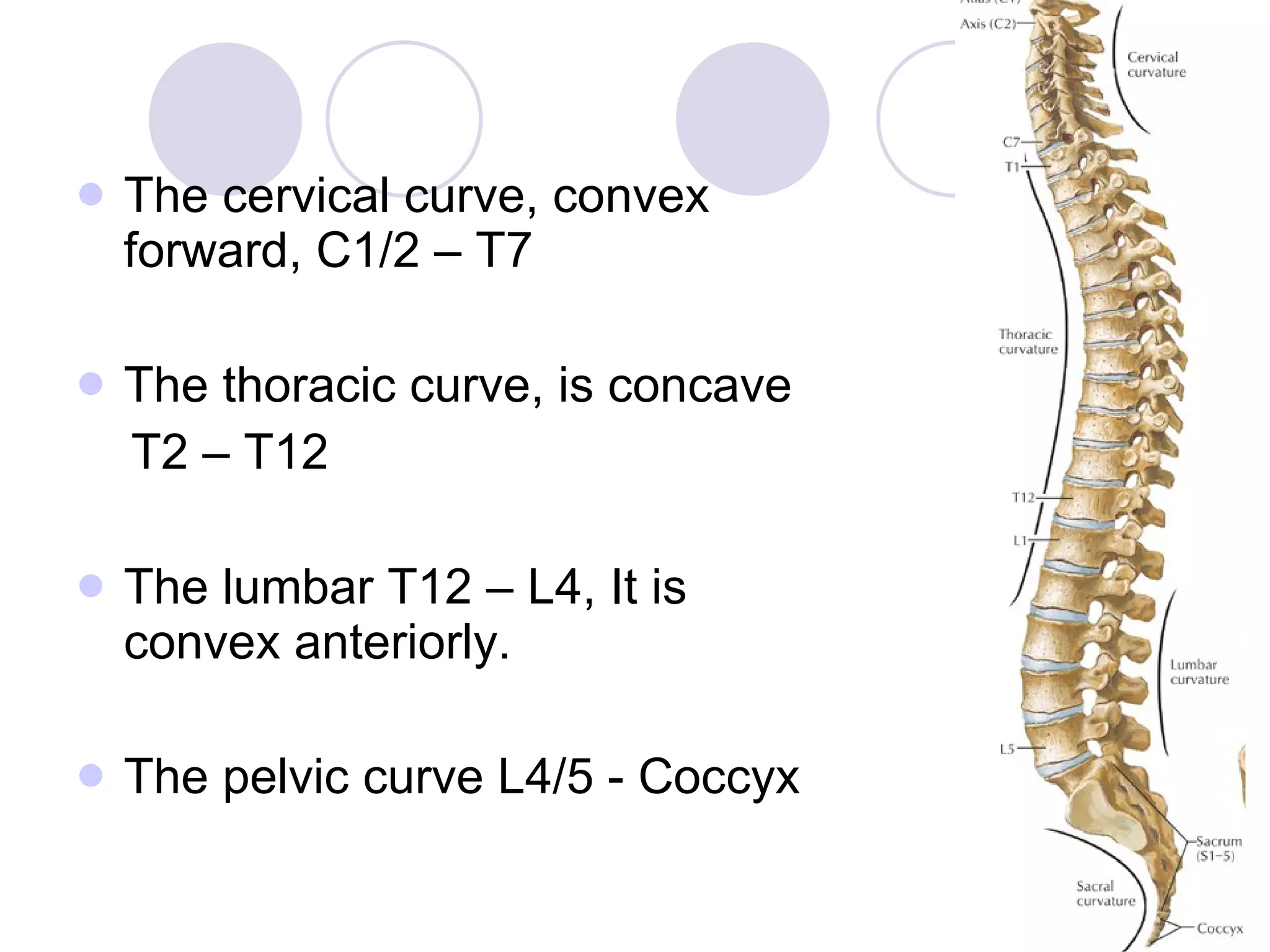
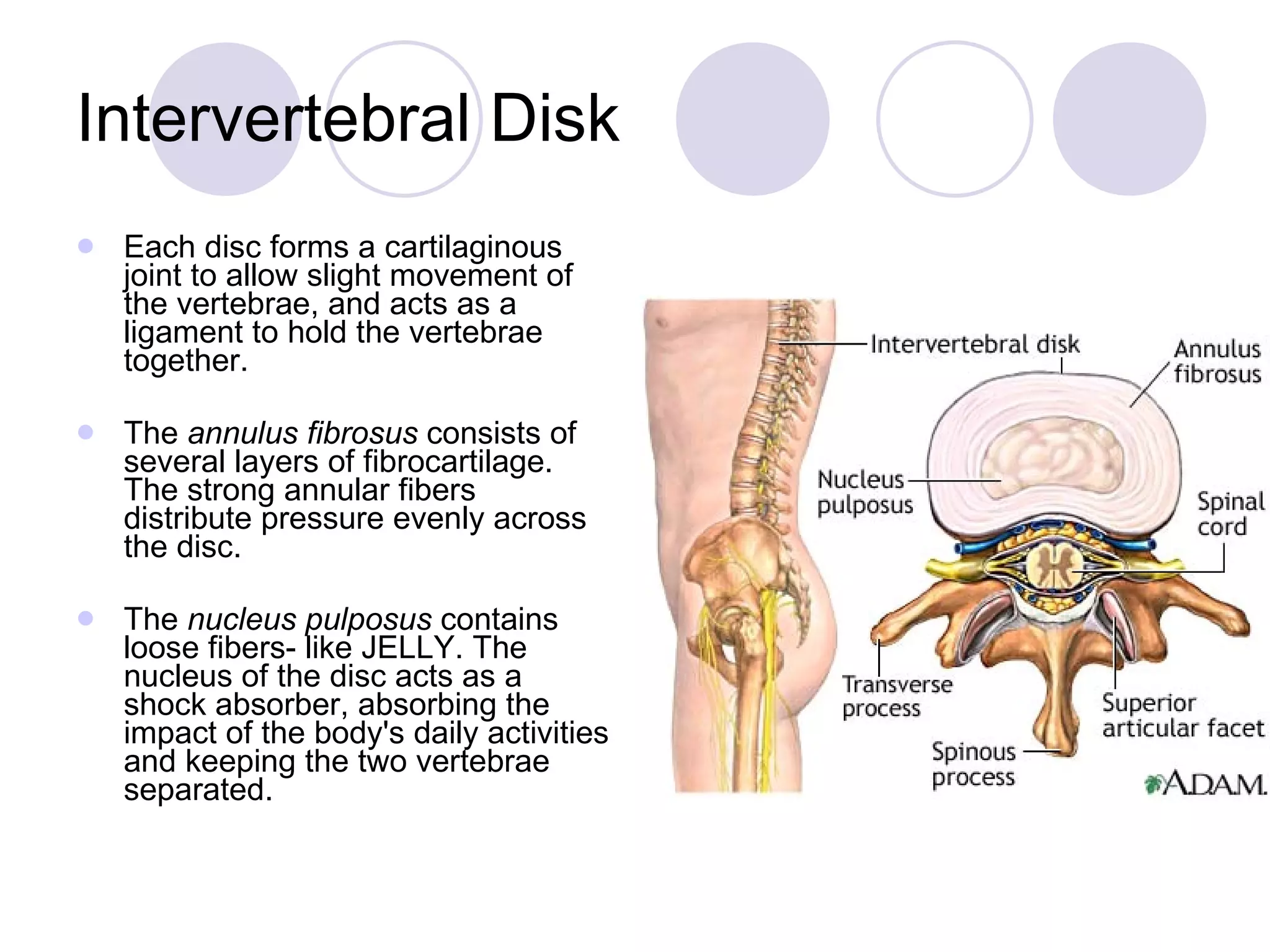
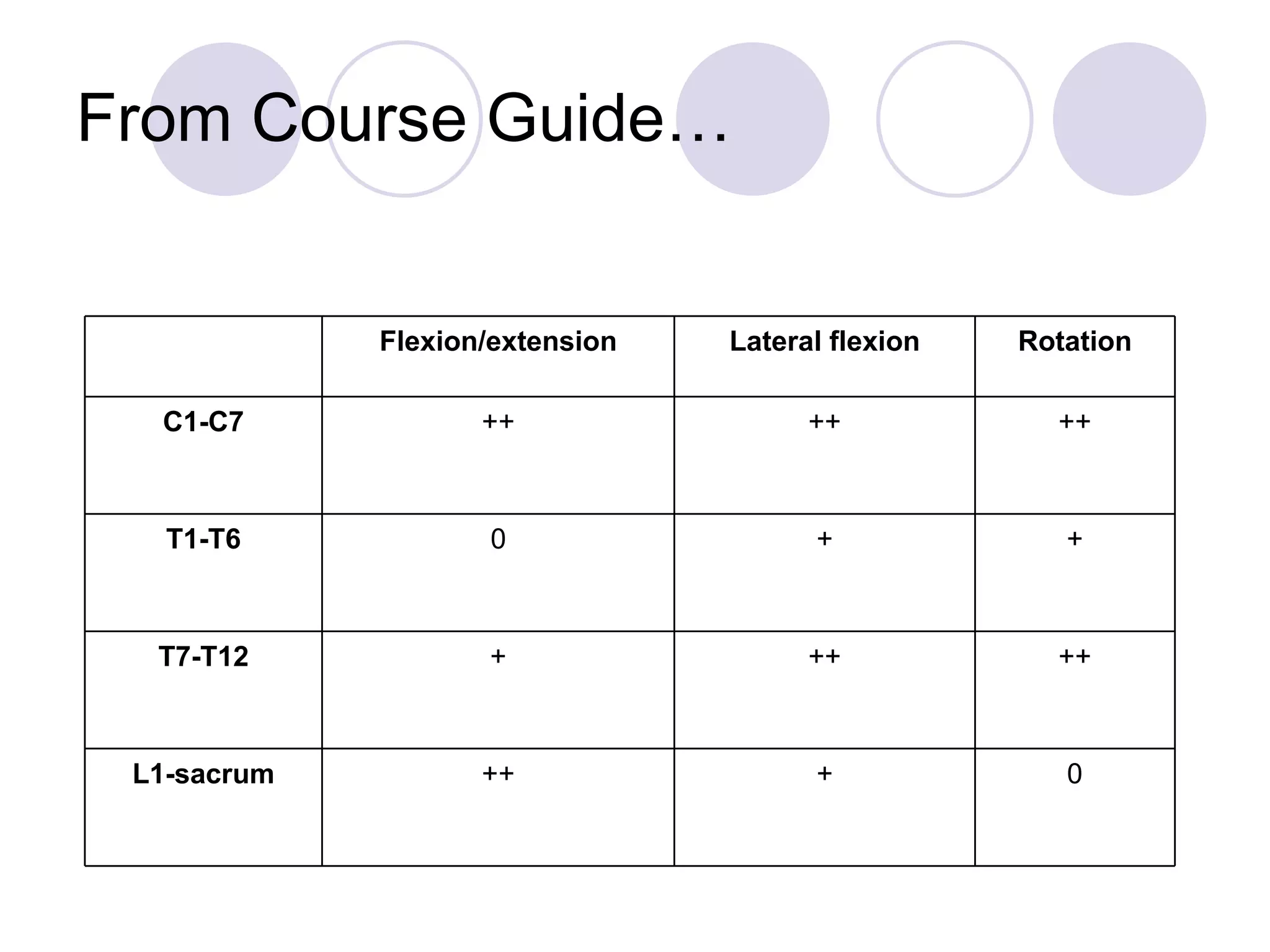
Description of spinal curvature and the role and injuries of intervertebral disks in spine health.
Factors contributing to common back pain, explanation of spinal mobility, and abnormalities like kyphosis.
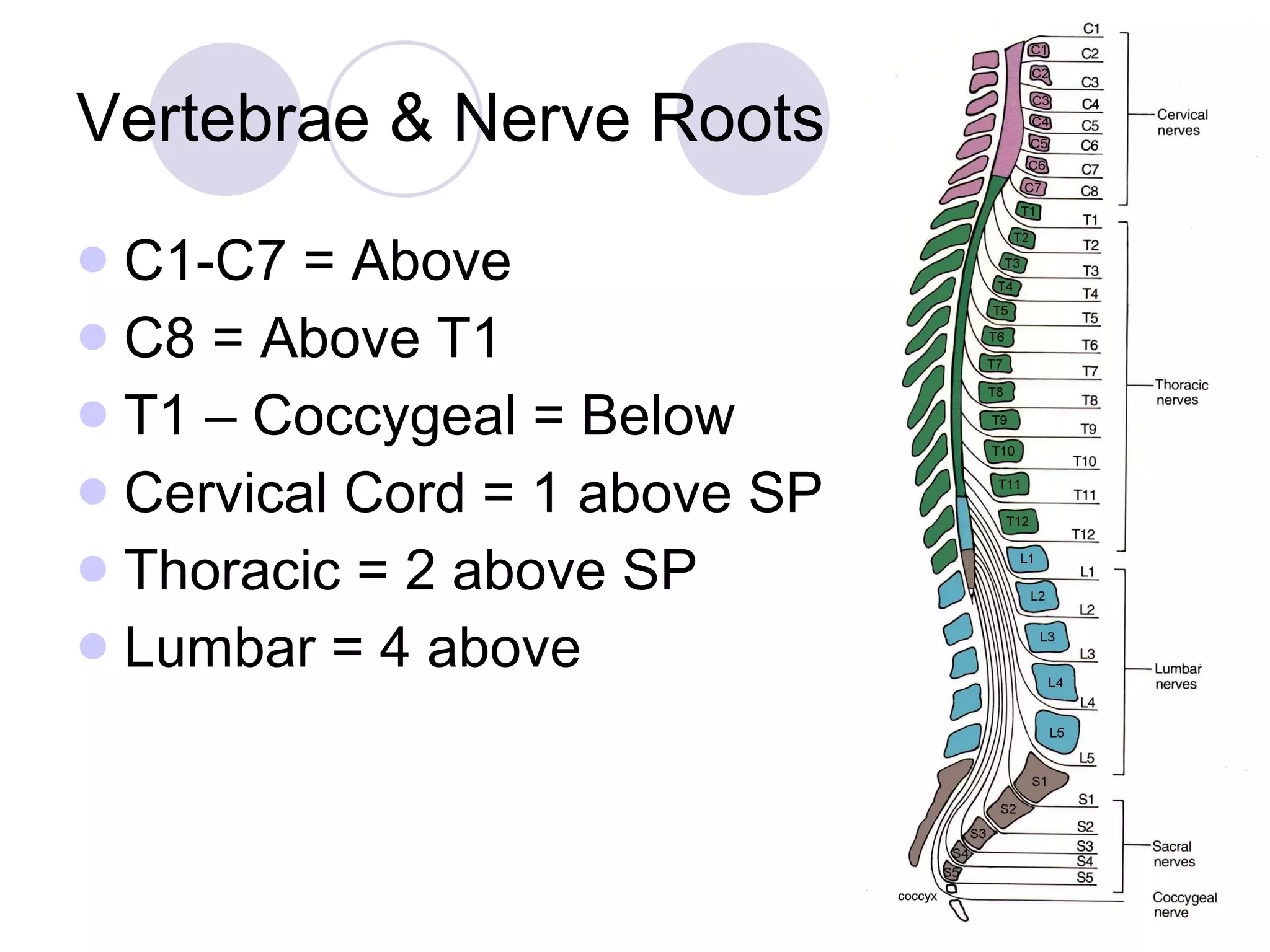
Indications for lumbar puncture, its risks, and the anatomy concerning nerve roots.
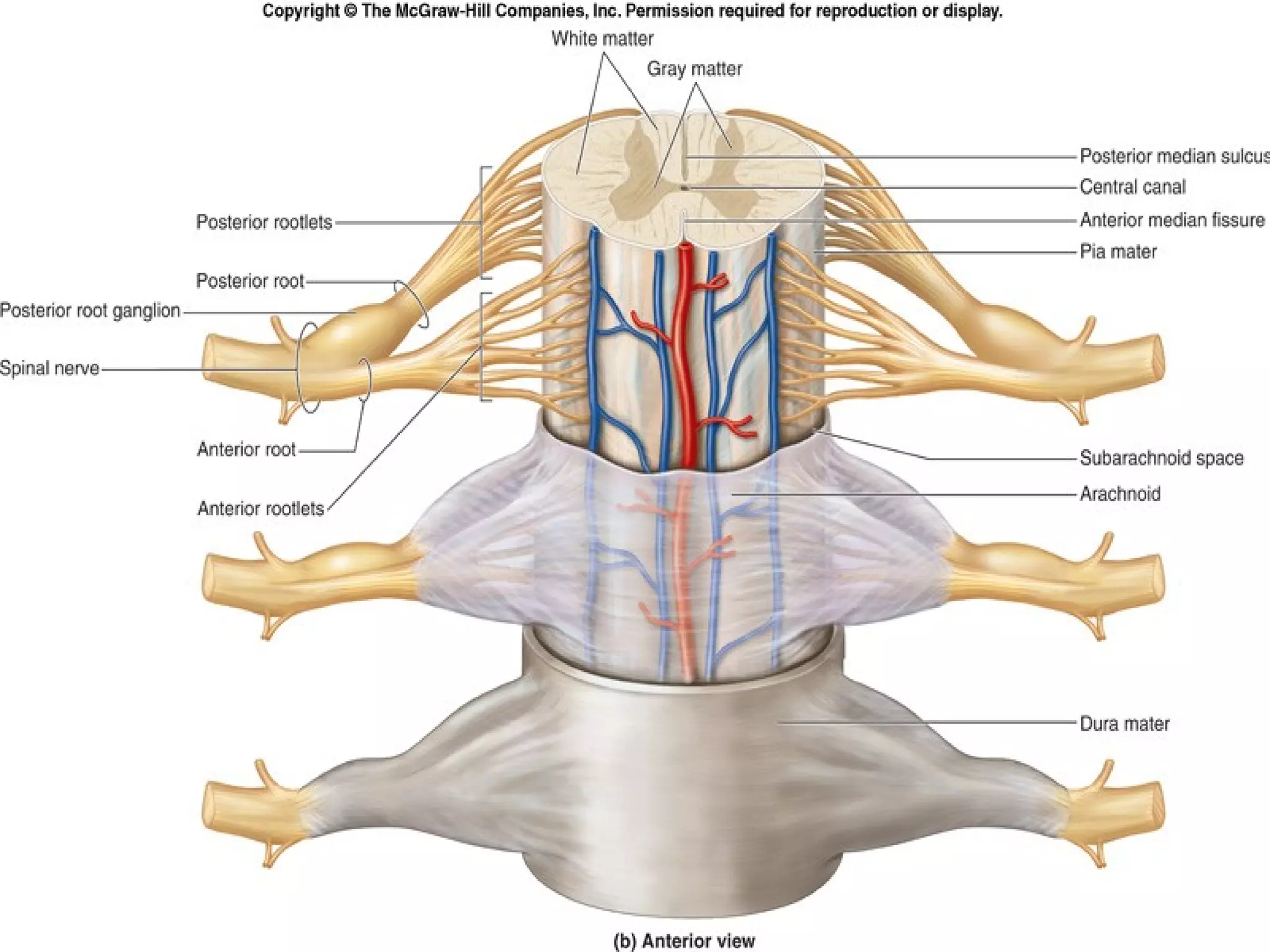
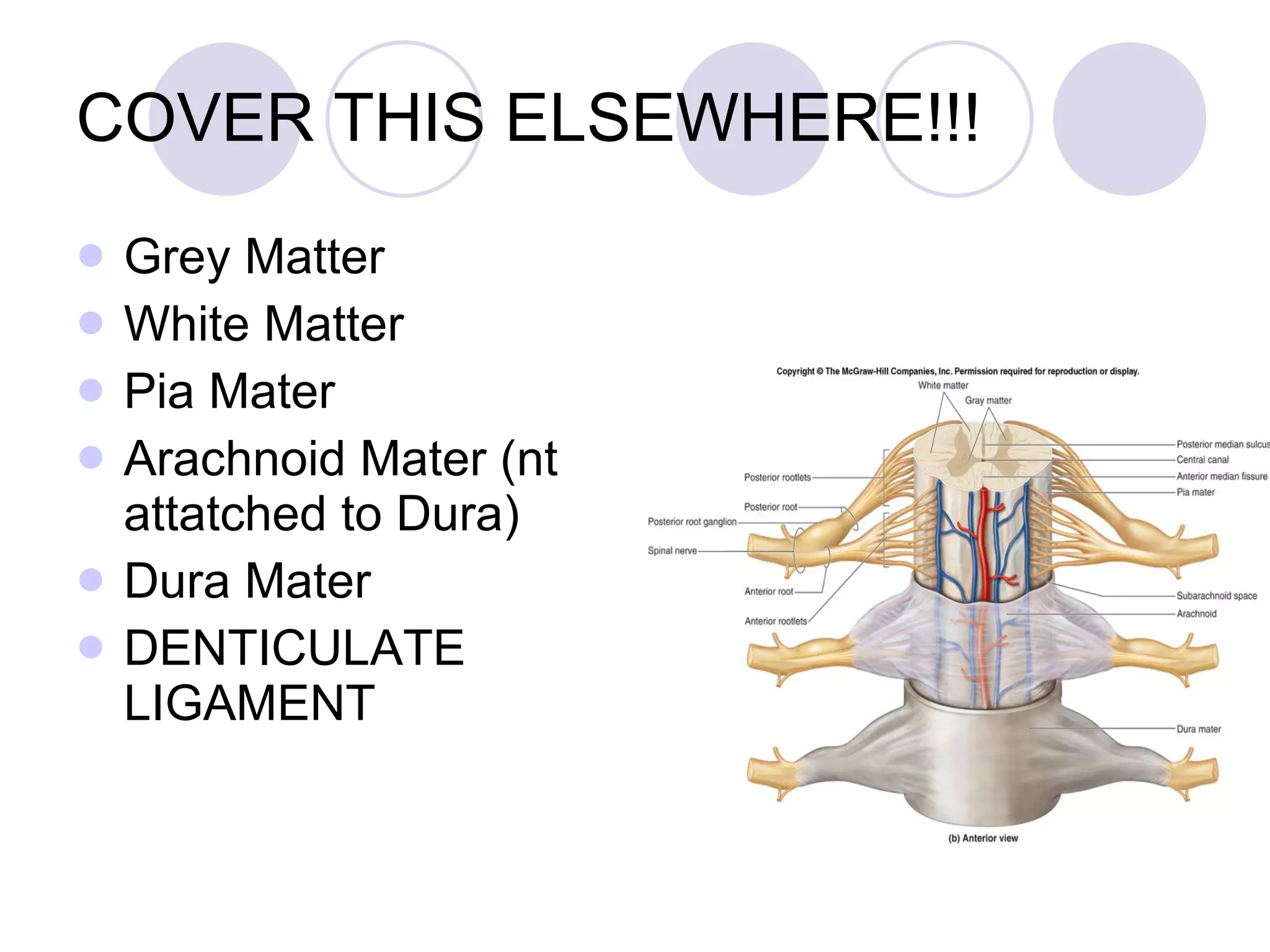
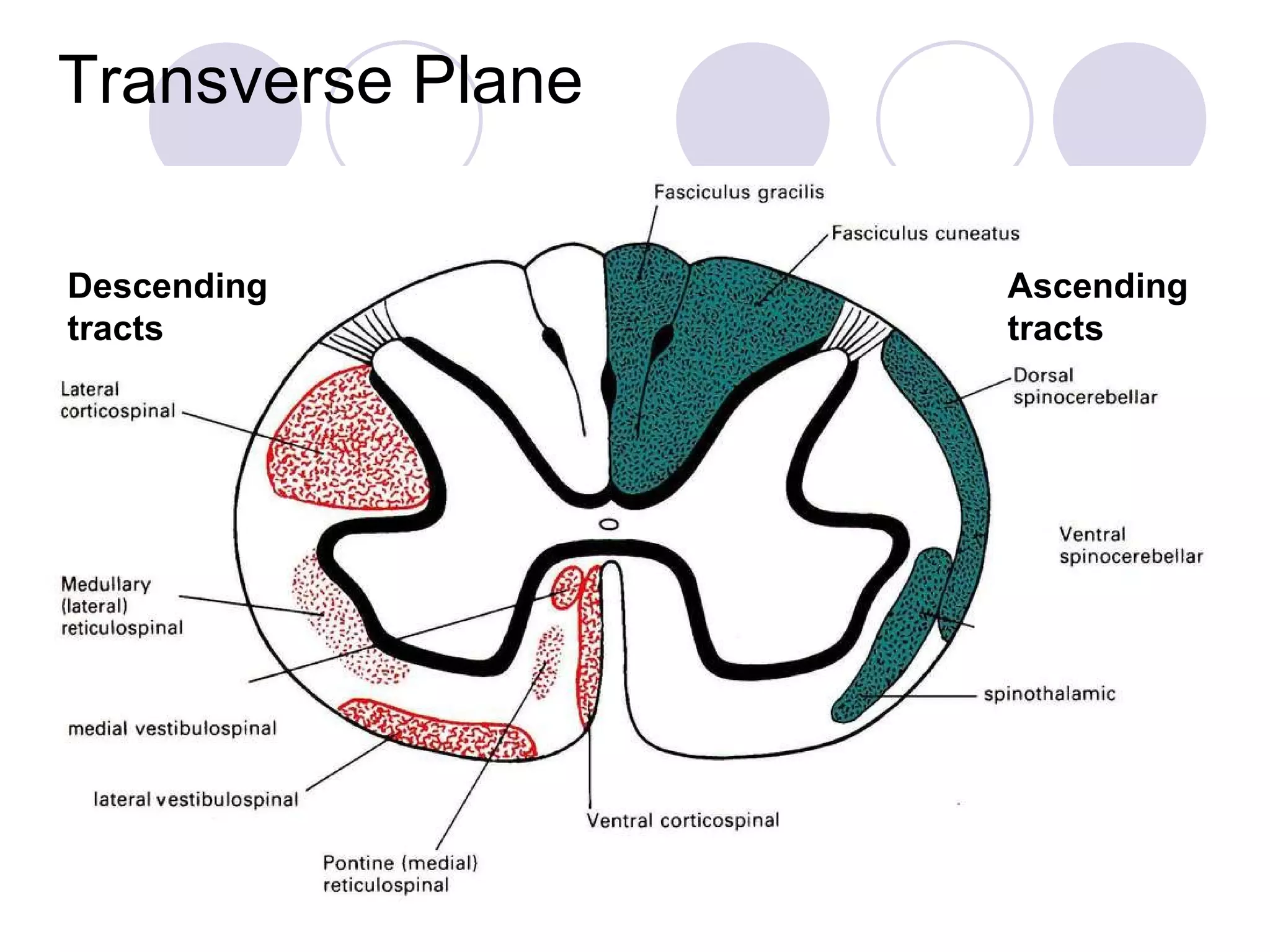
Components of the spinal cord, including grey and white matter, ascending and descending tracts.
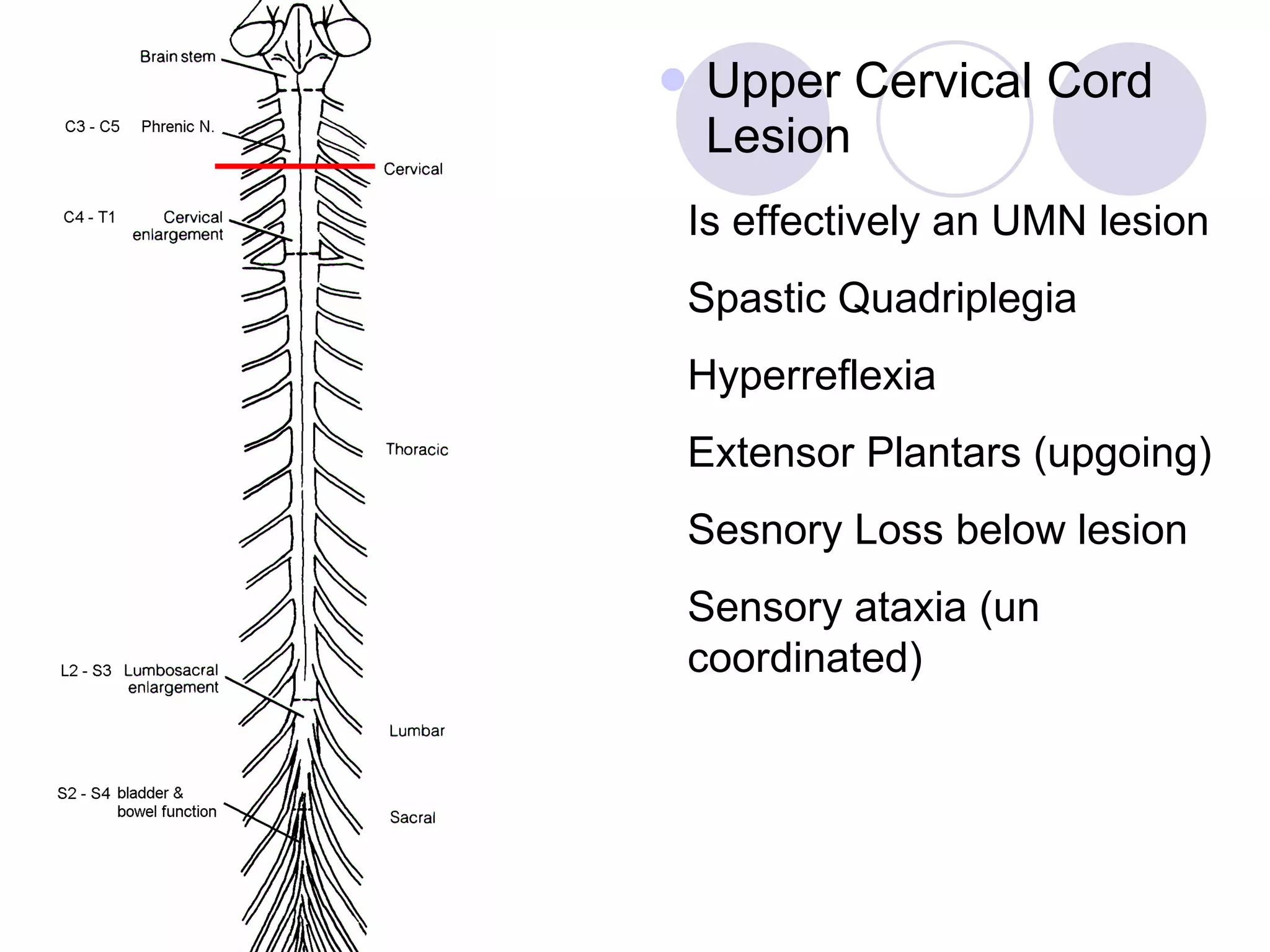
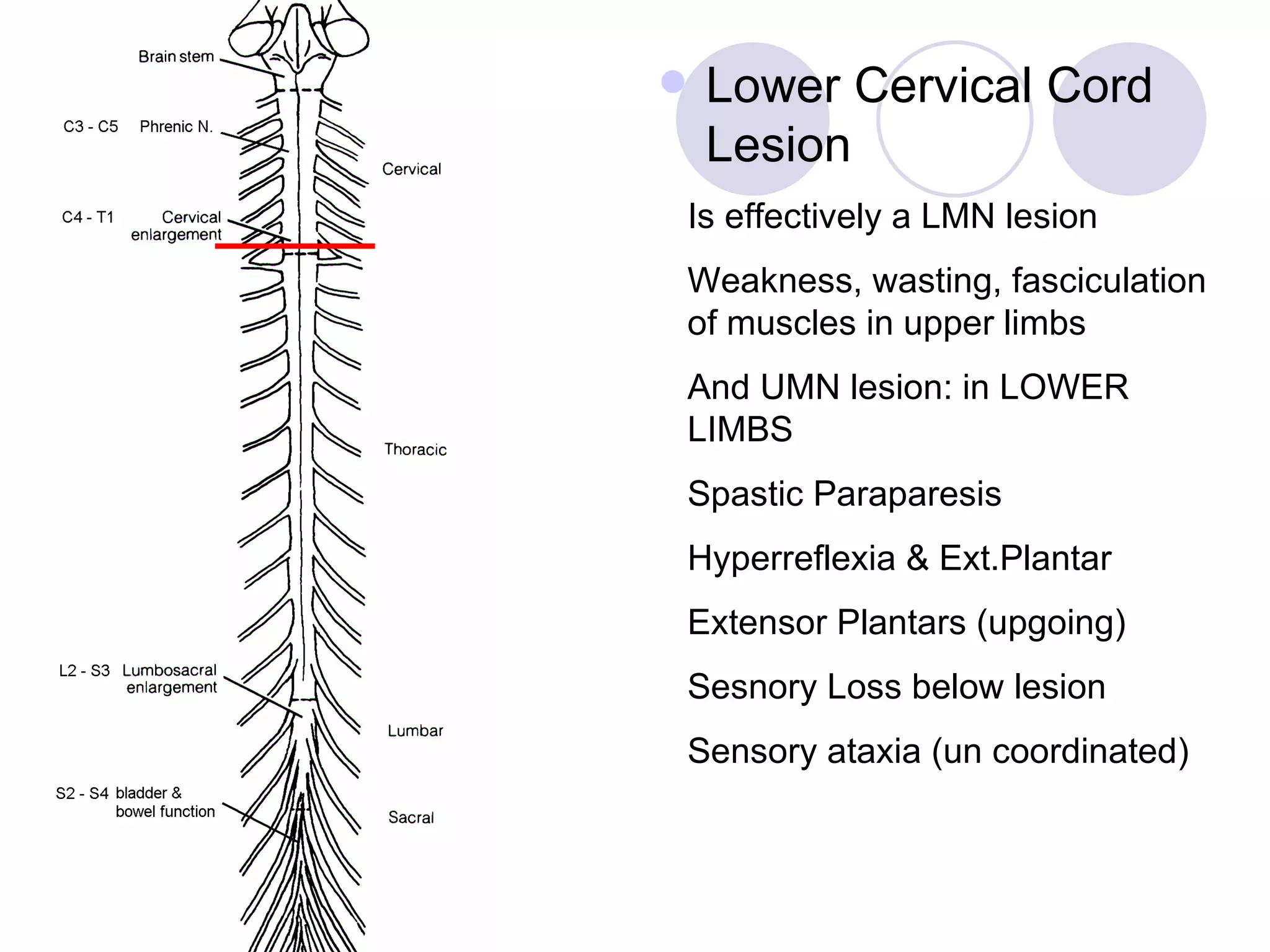
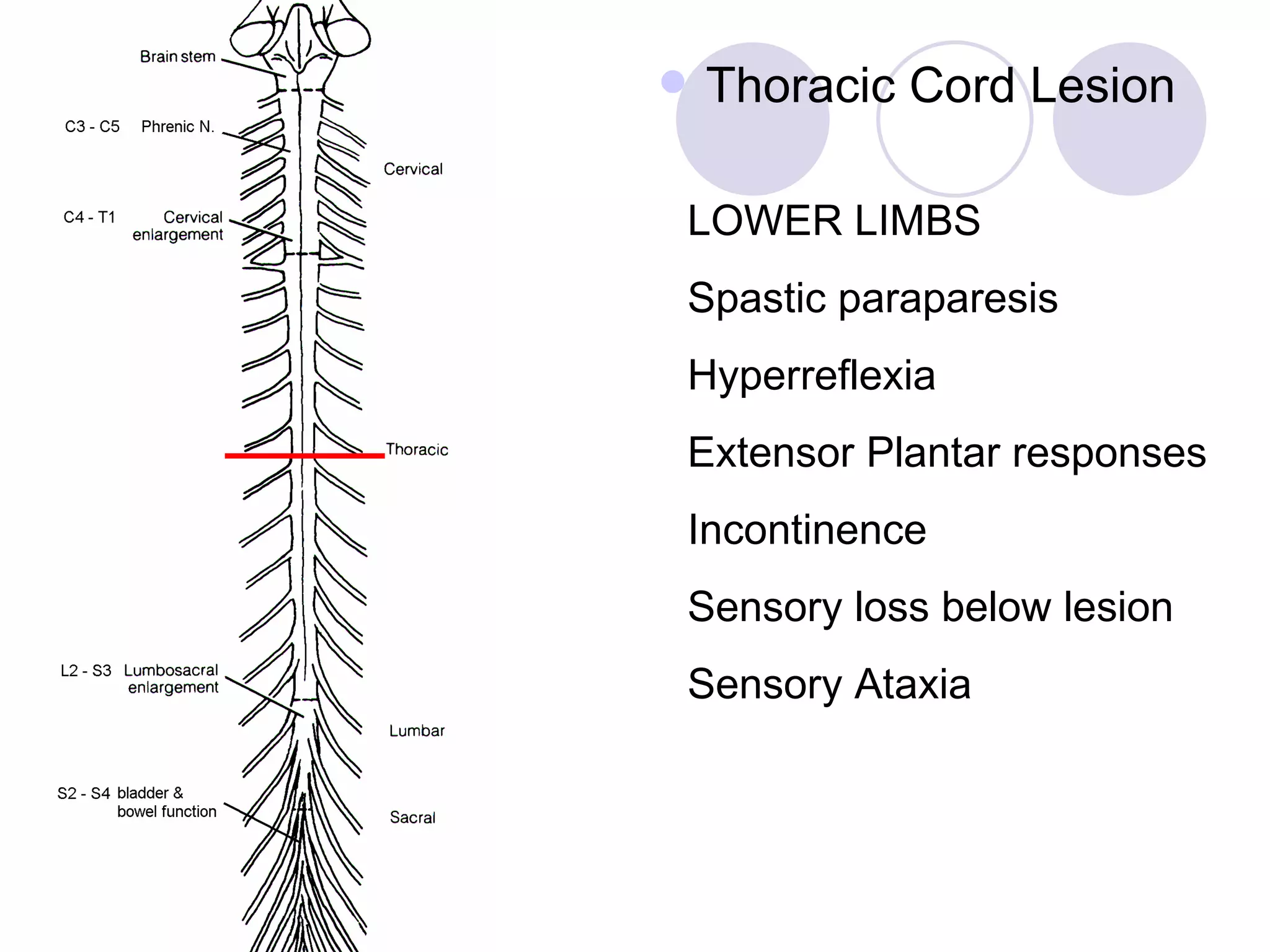
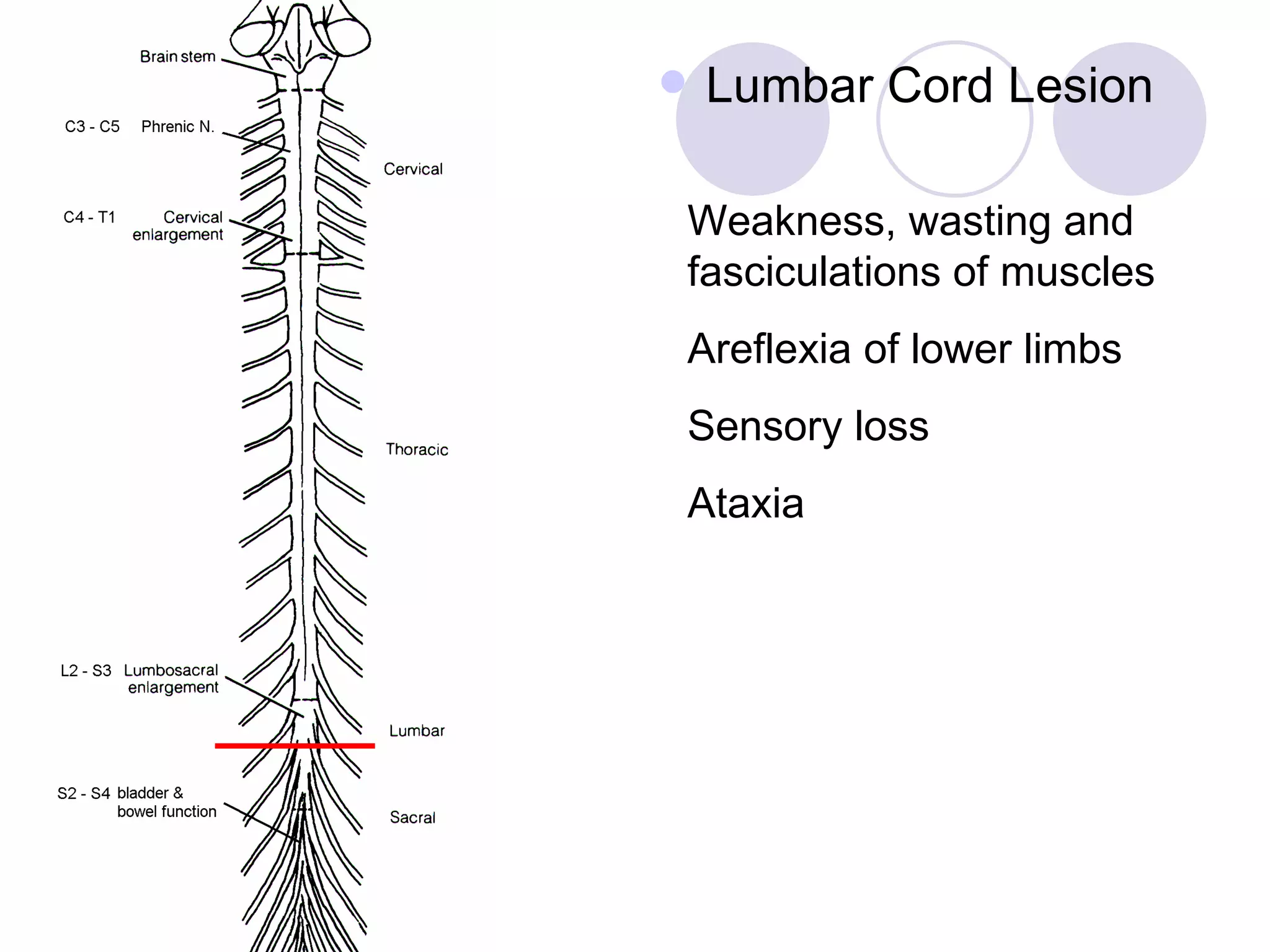
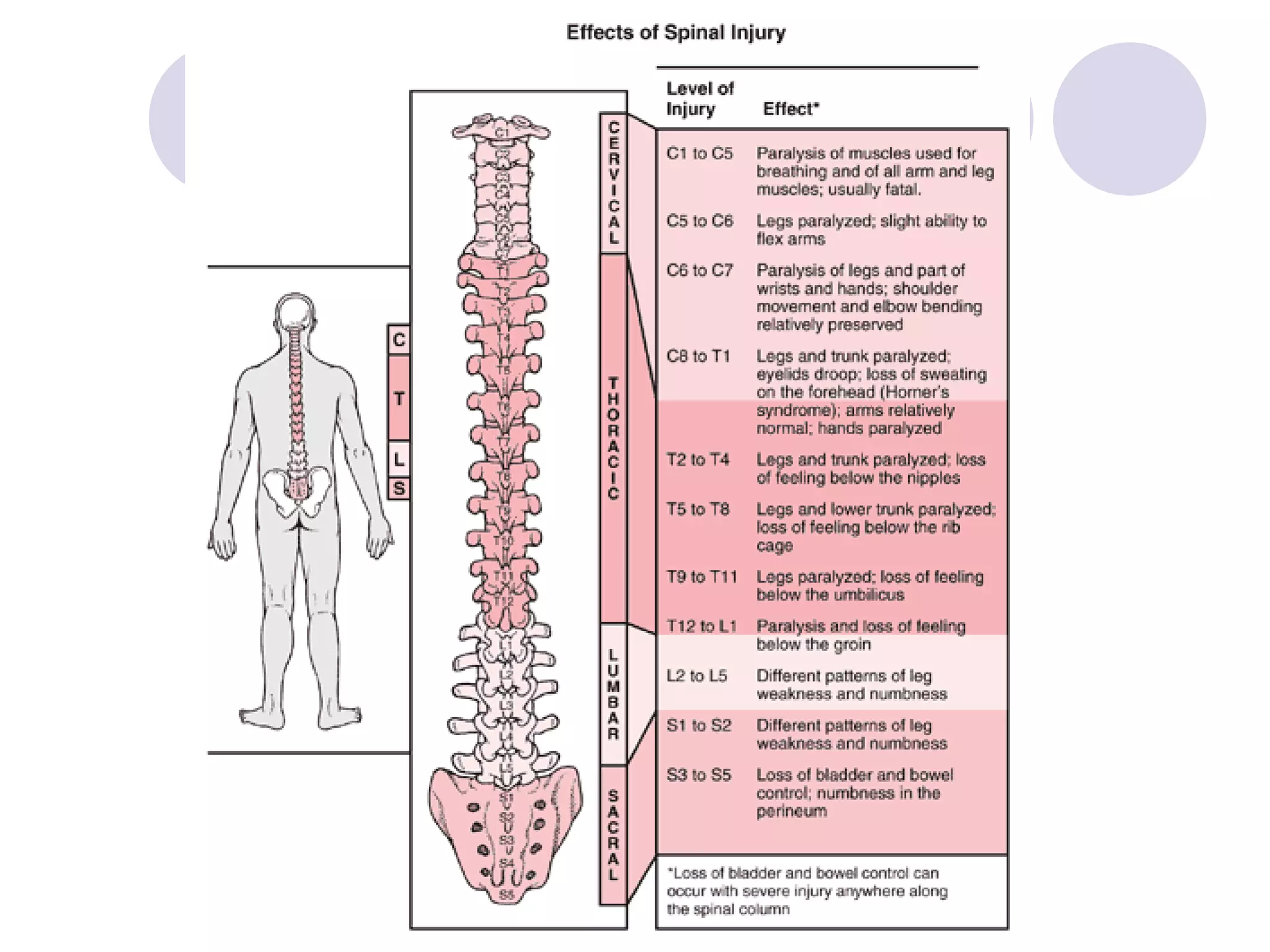
Impacts of spinal trauma, lesions, and strategies to recognize upper and lower cord injuries.
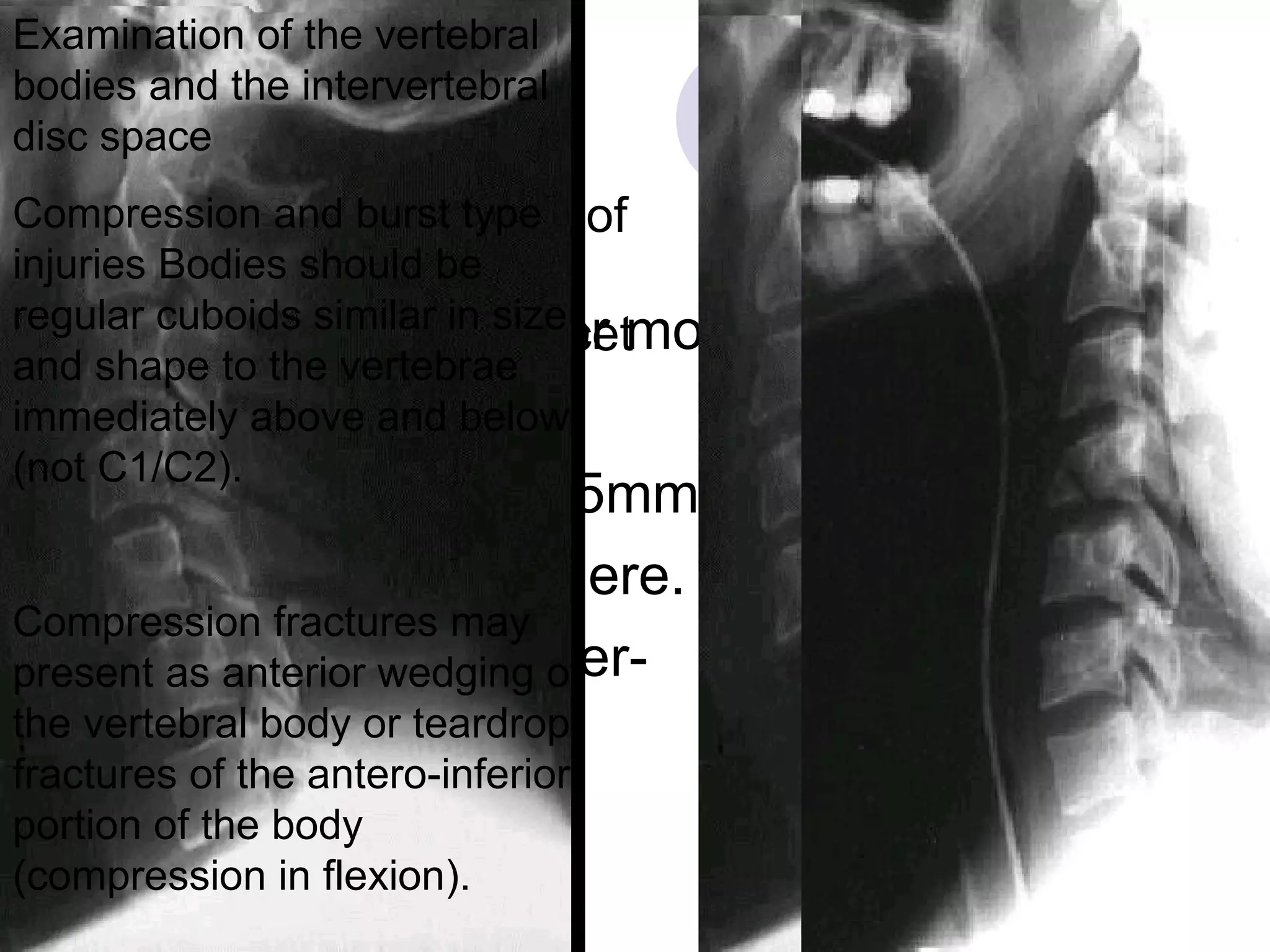
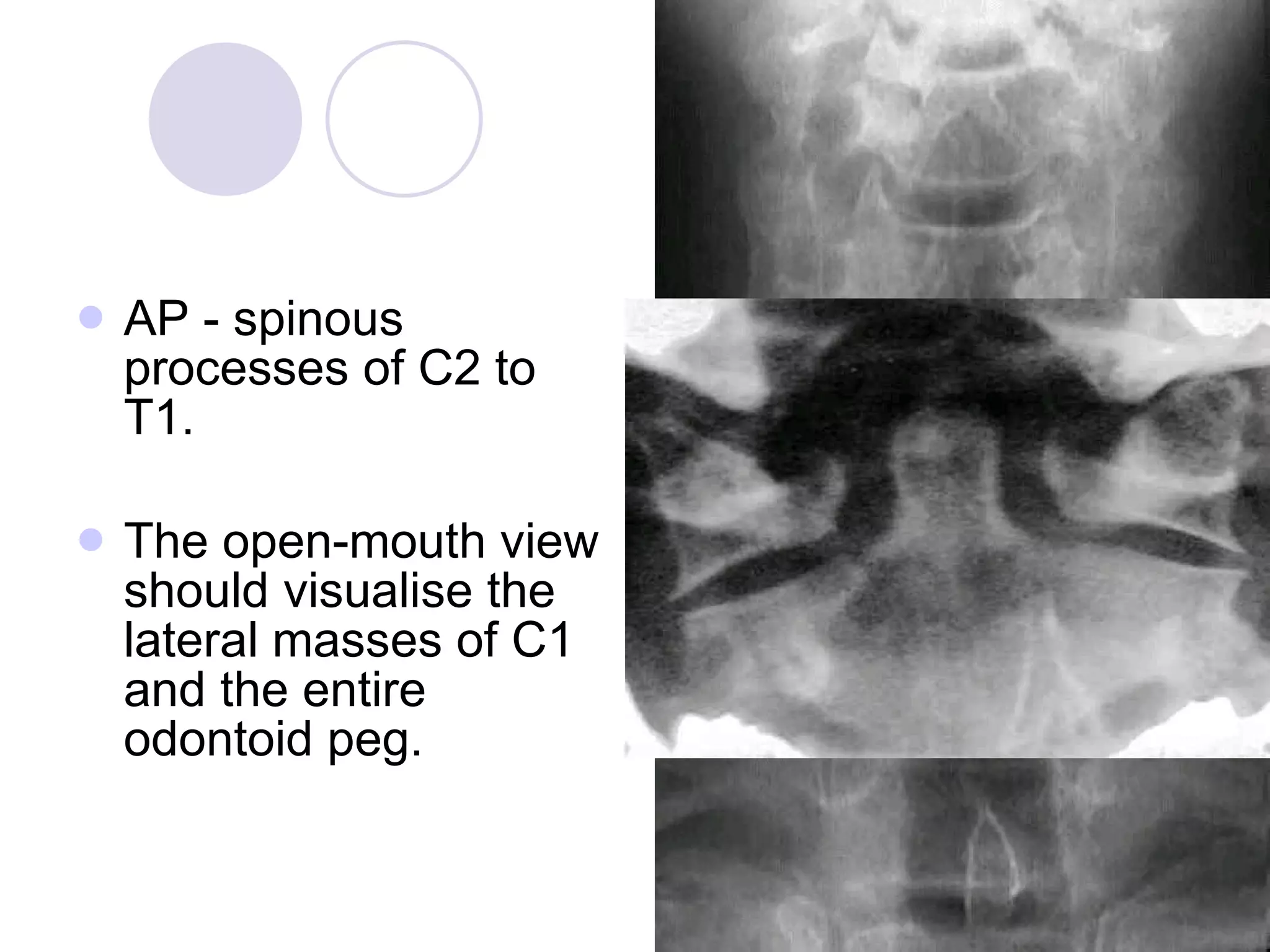
Priorities in spinal trauma management, including immobilization techniques and imaging protocols.















































![[3] The Back and ANS.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/3thebackandans-230325182407-aaf75a6c-thumbnail.jpg?width=640&height=640&fit=bounds)







































