Downloaded 572 times

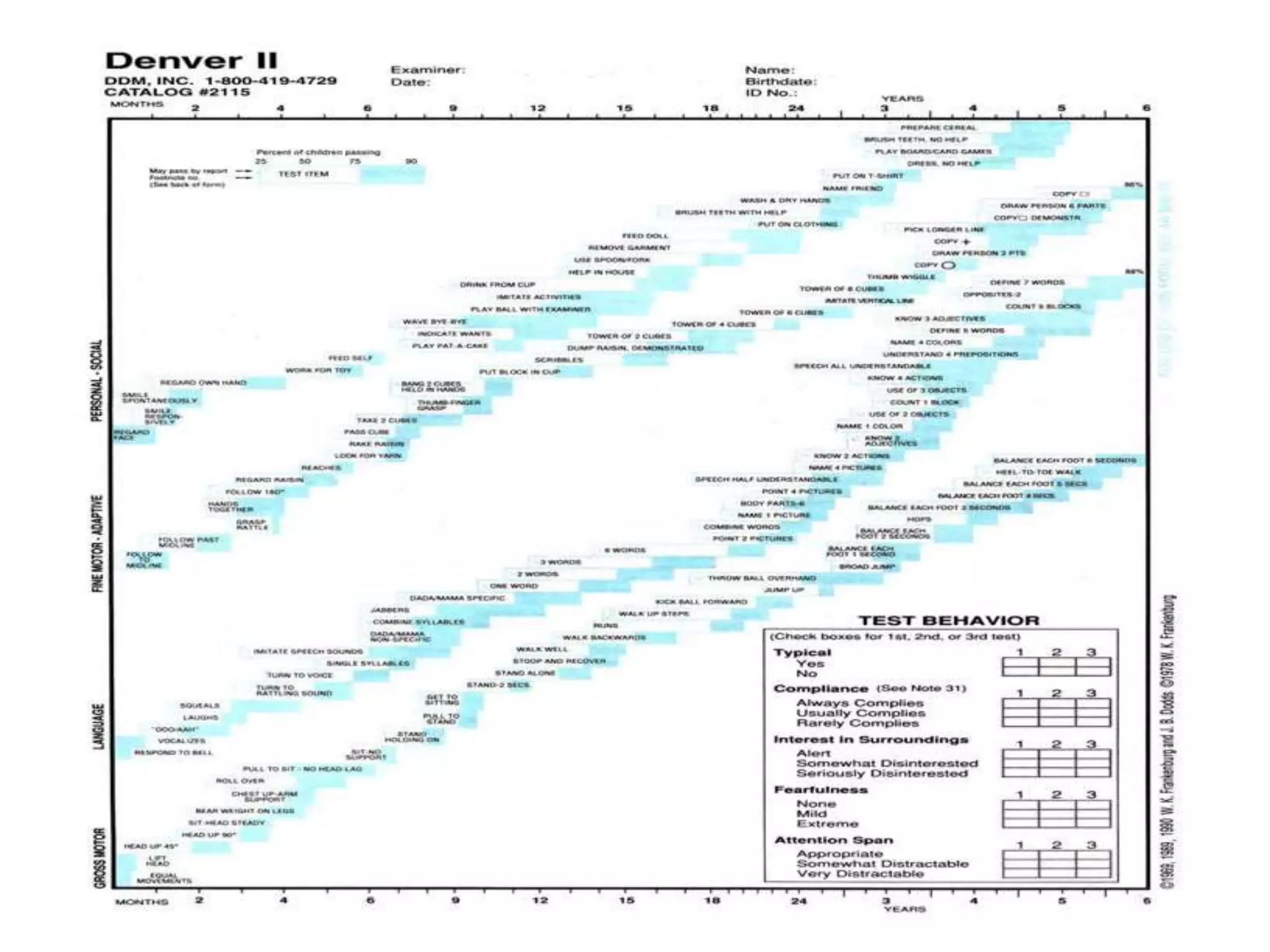
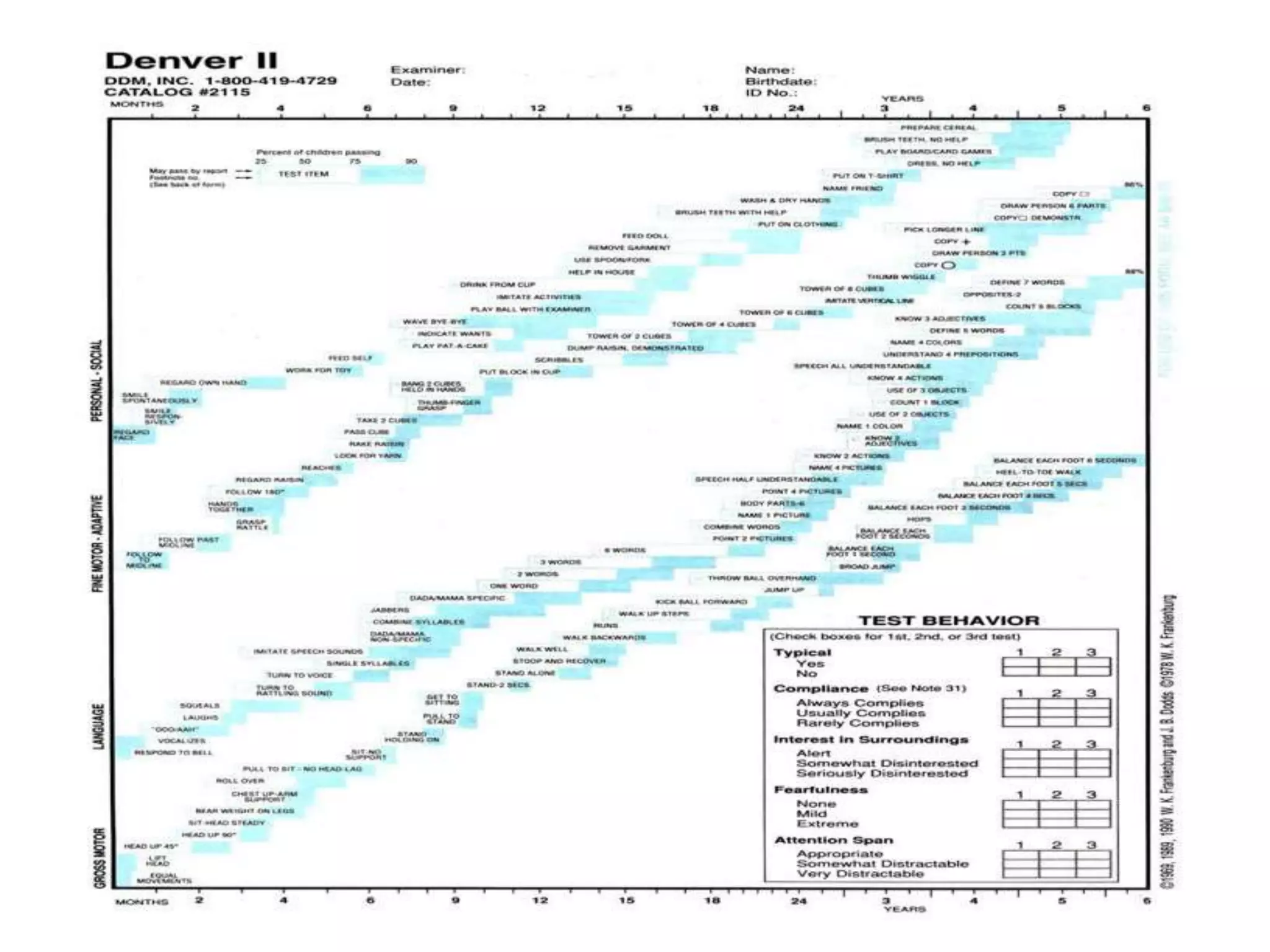
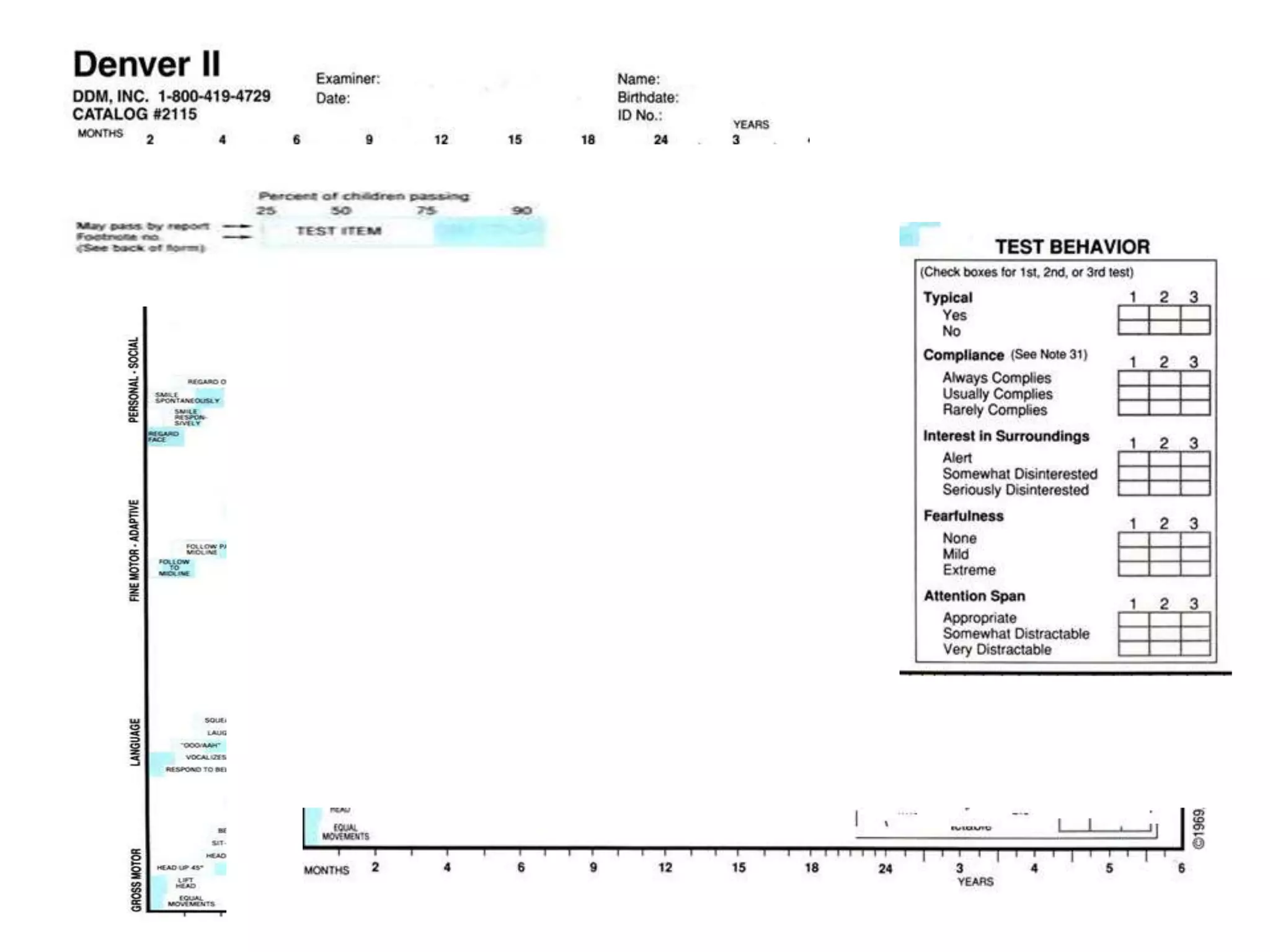
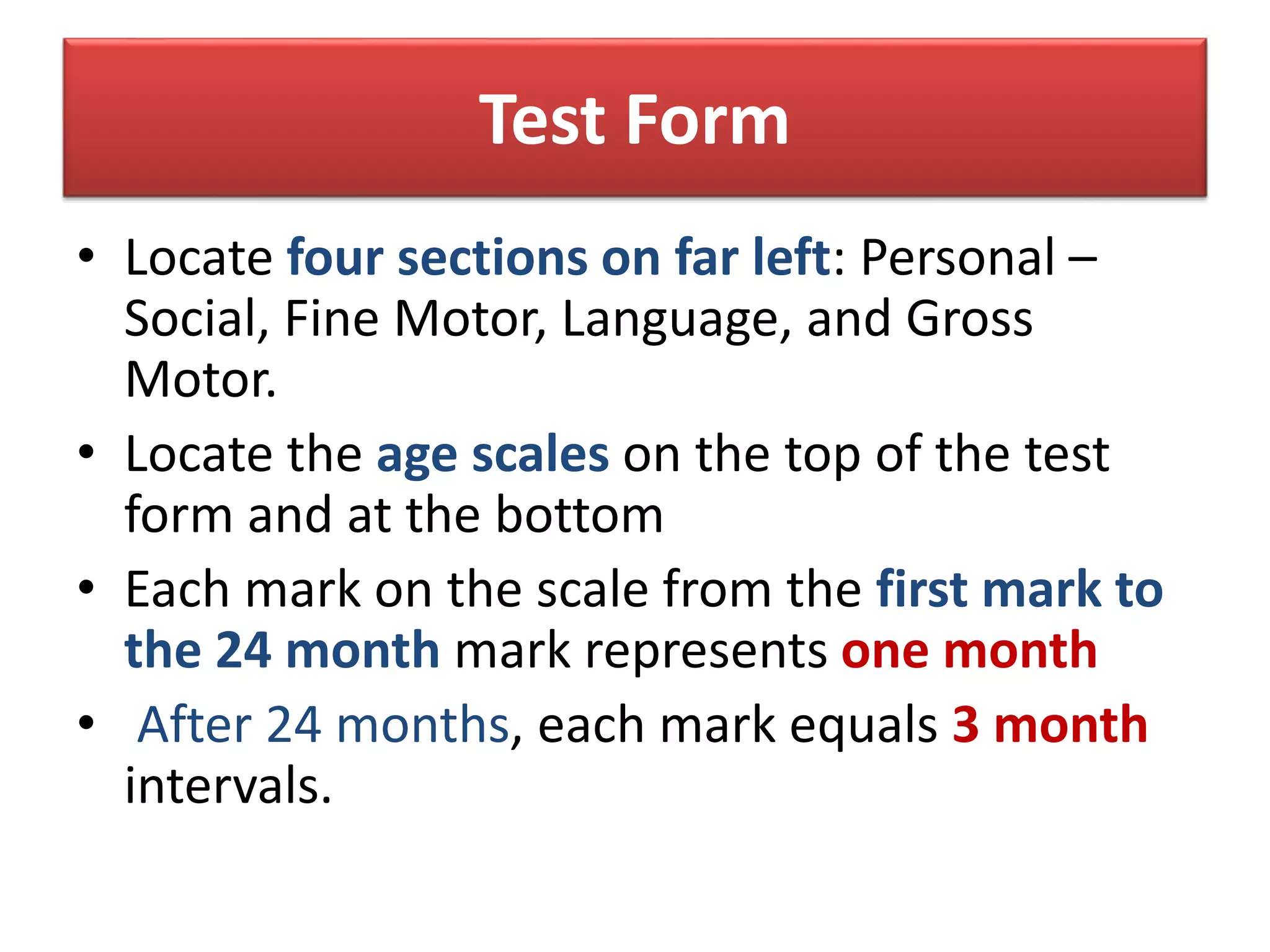


The document provides information about the Denver-II developmental screening test, including its history, administration, scoring, and interpretation. Some key points: - The Denver-II screens children ages 0-6 and assesses personal-social, fine motor, language, and gross motor development. It identifies potential developmental delays. - The test consists of 125 items across the four developmental domains. It is administered through child activities and caregiver reports. - Responses are scored as pass, fail, no opportunity, or refusal. Delays or multiple cautions on the scoring sheet may indicate need for further assessment. - Interpretation categories are normal, suspect, or untestable. Referral is considered for























































































