Downloaded 491 times
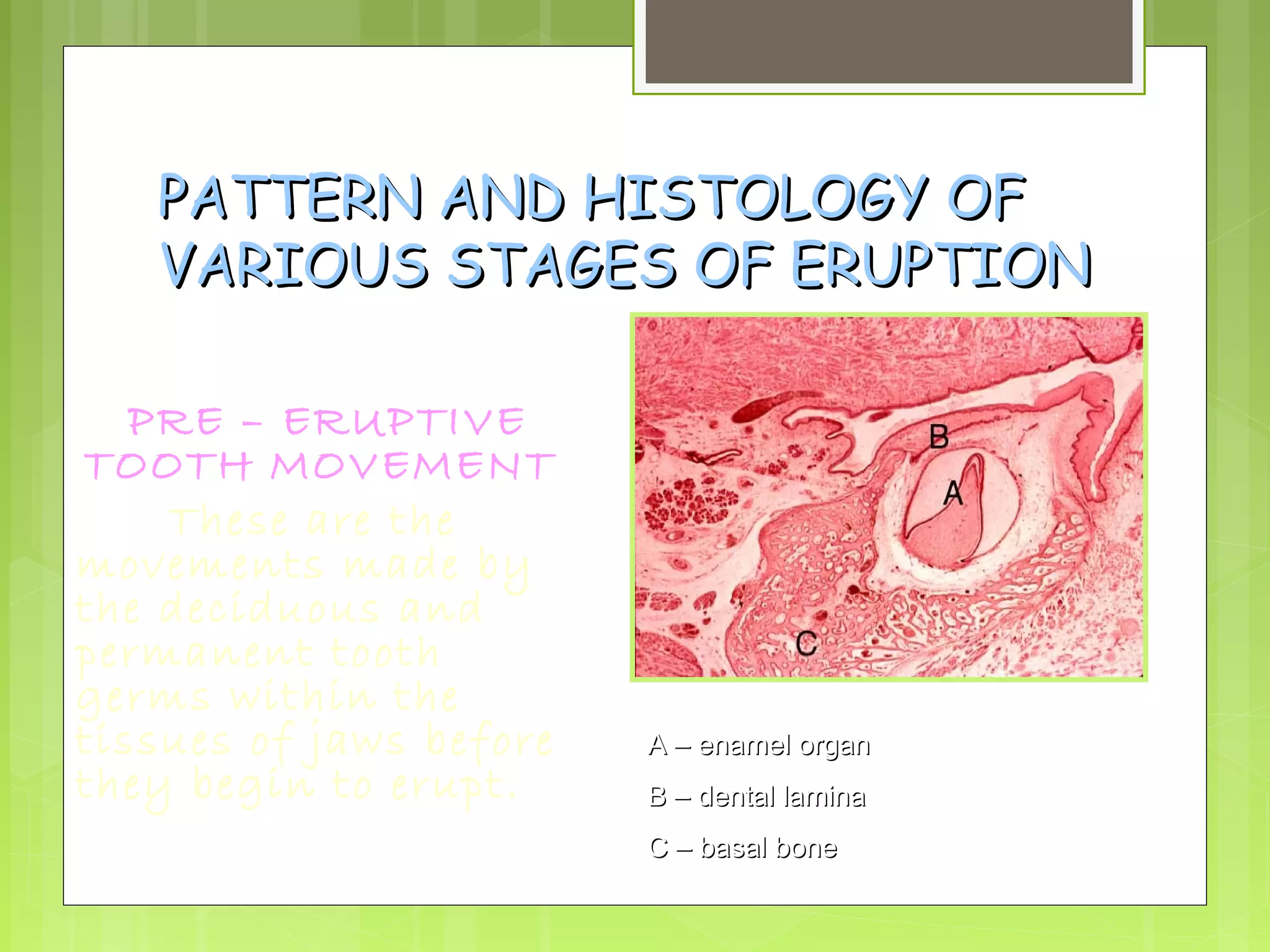

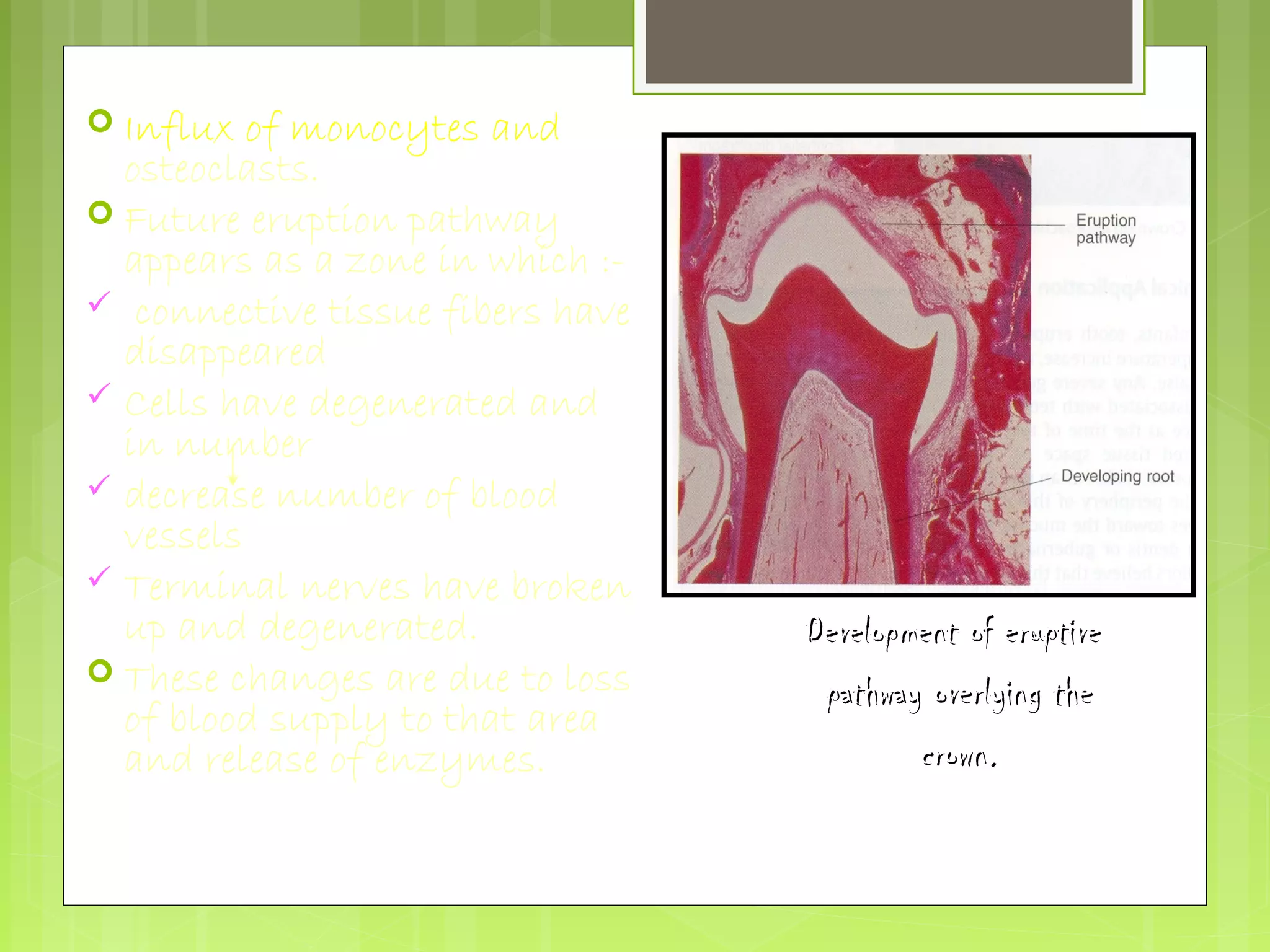
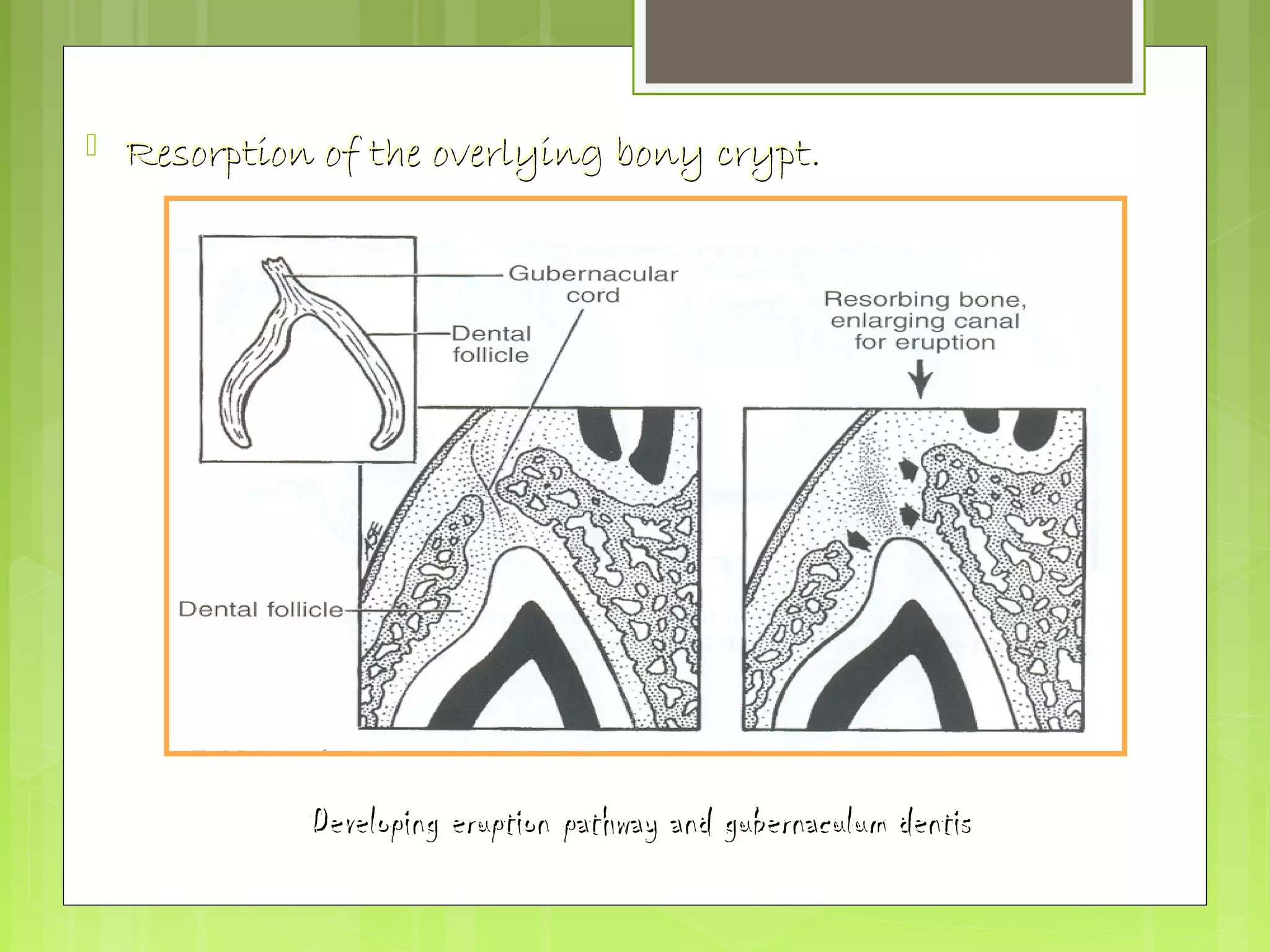
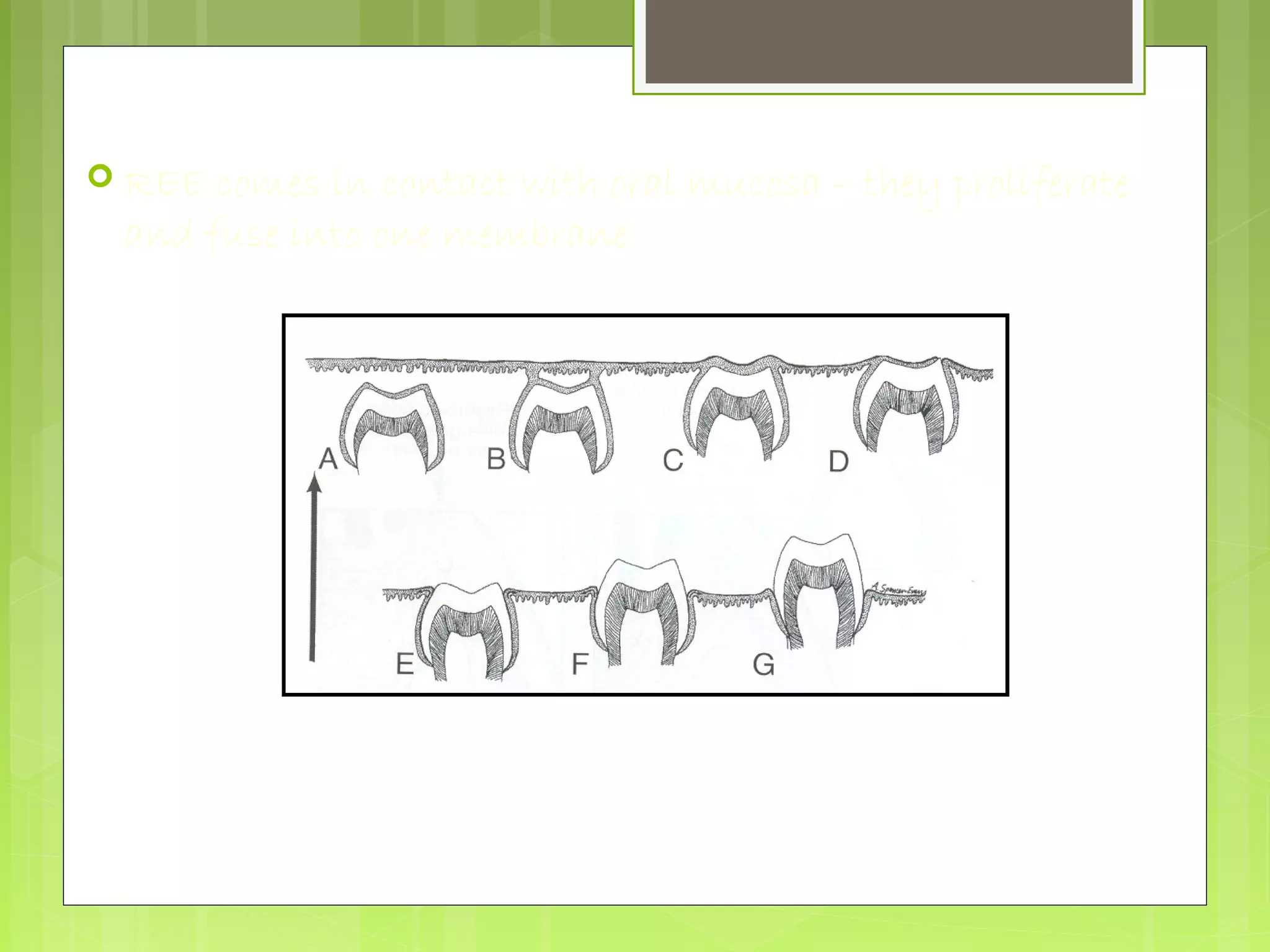
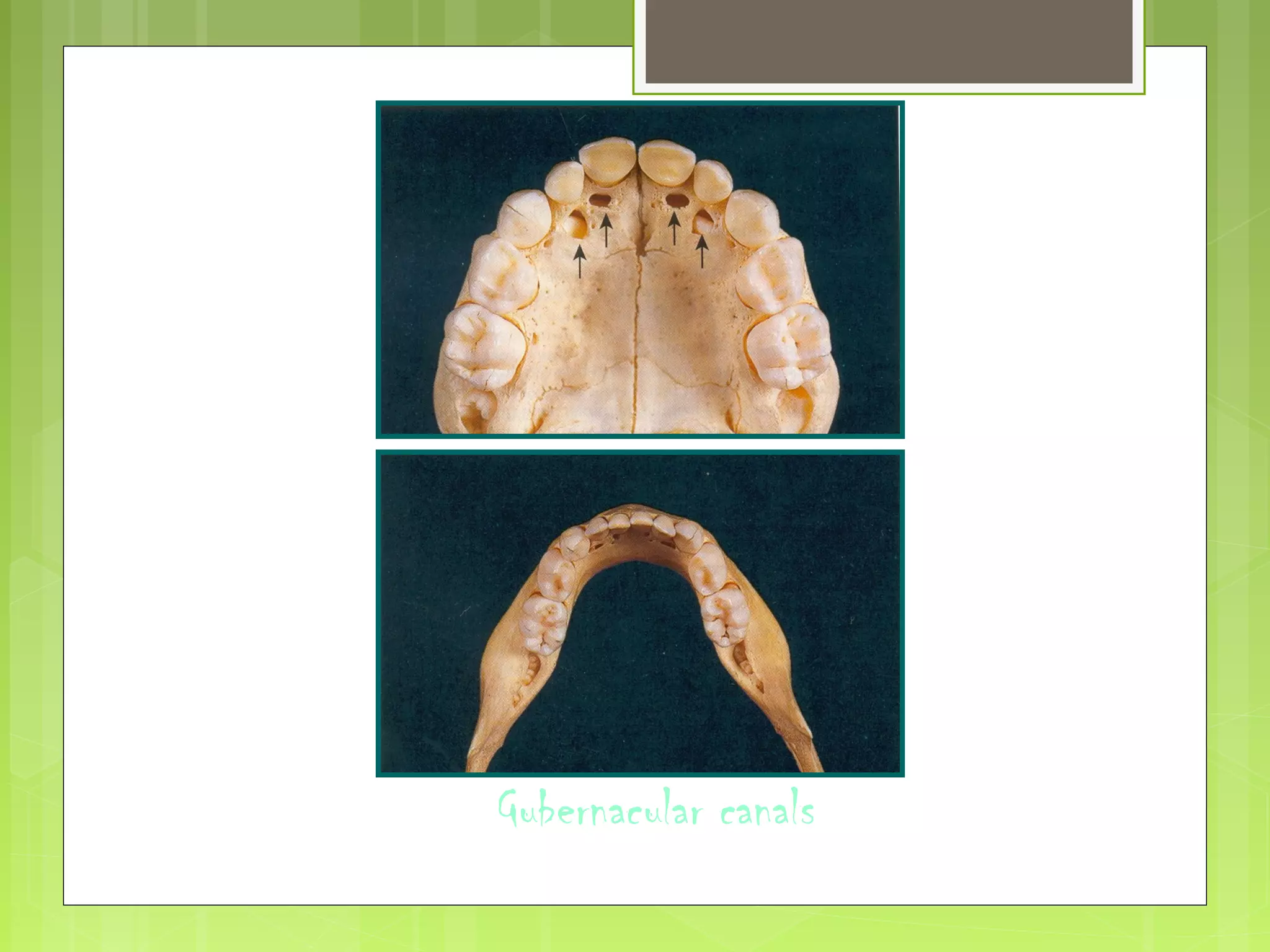
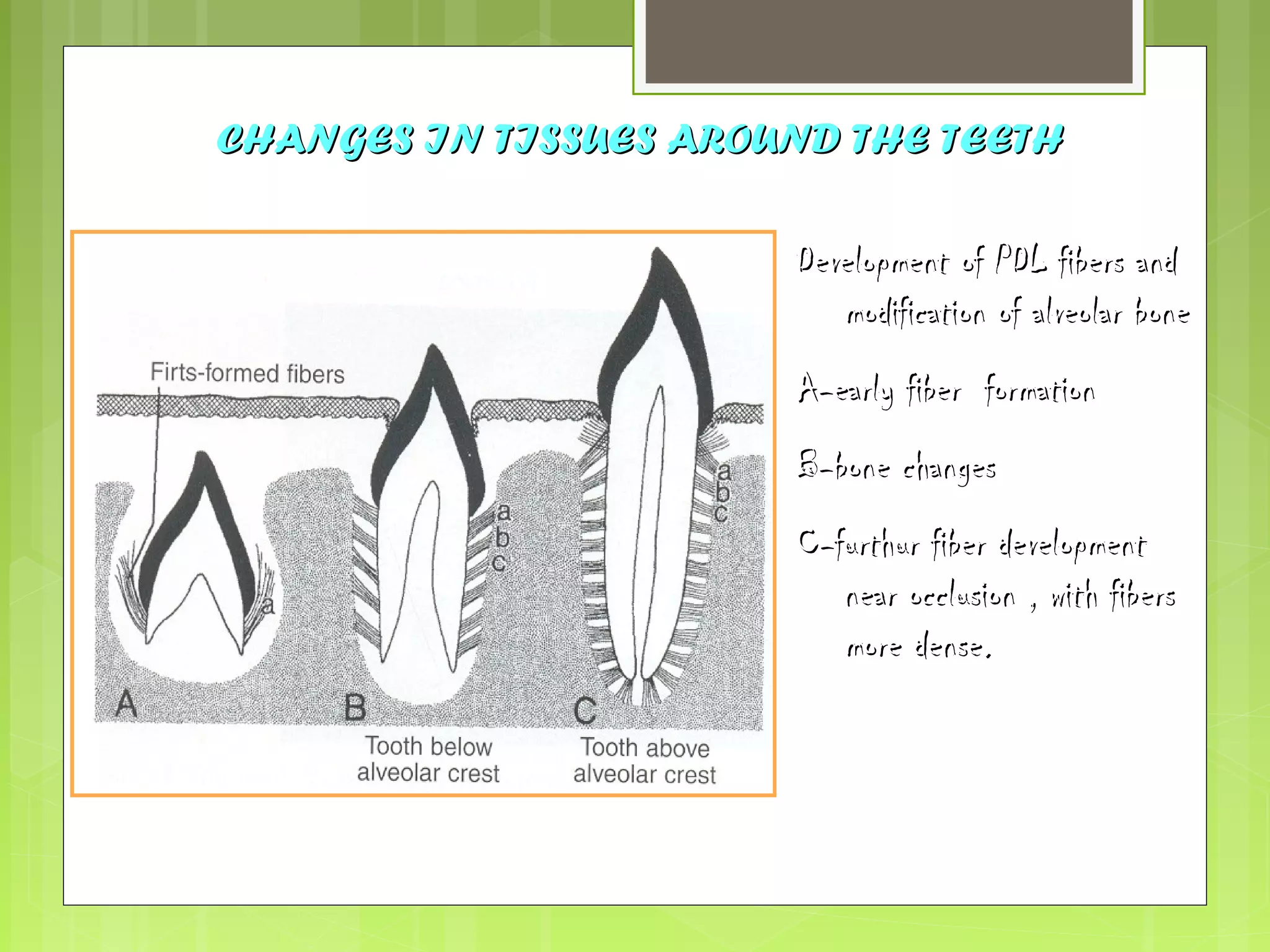
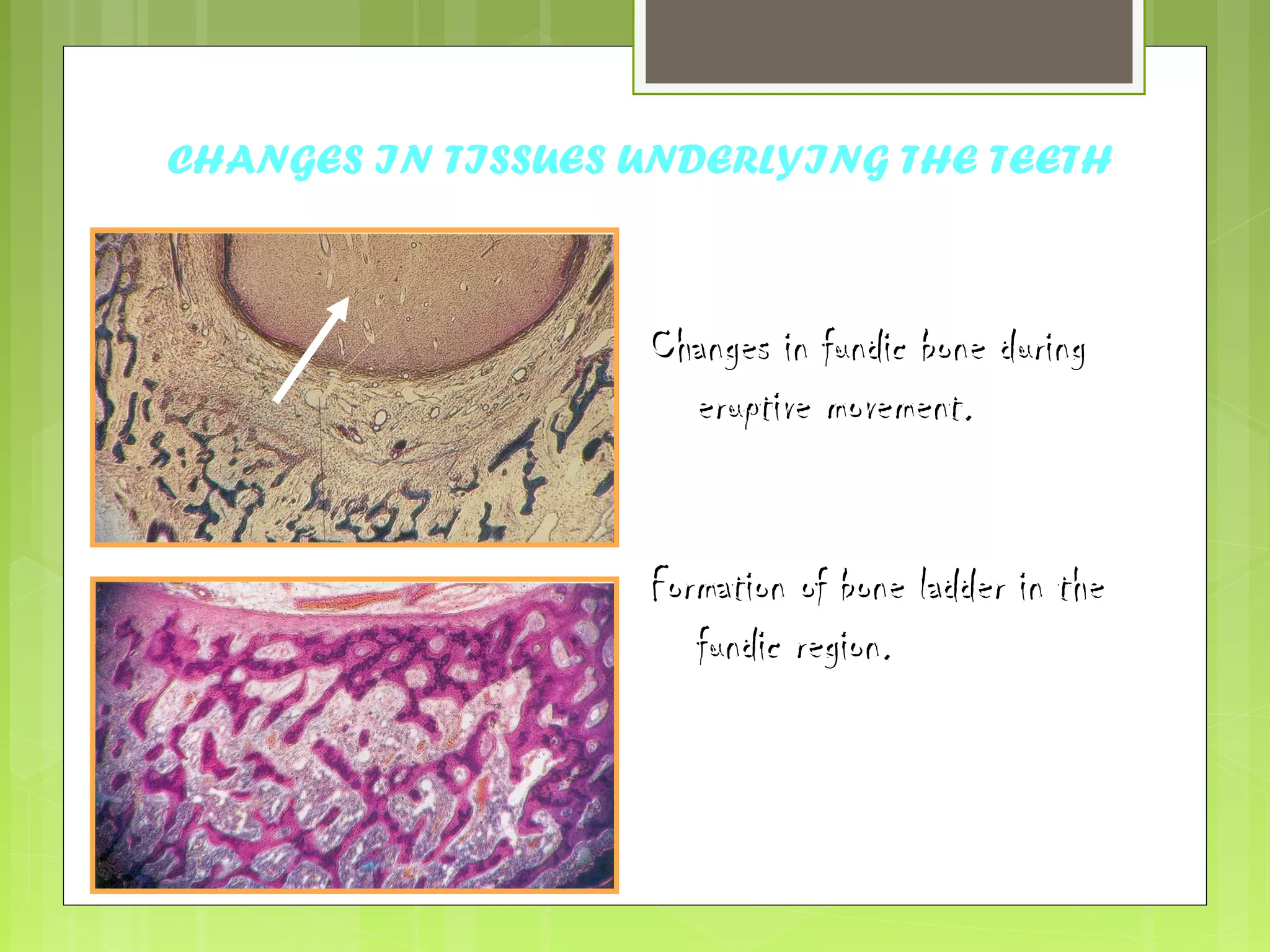

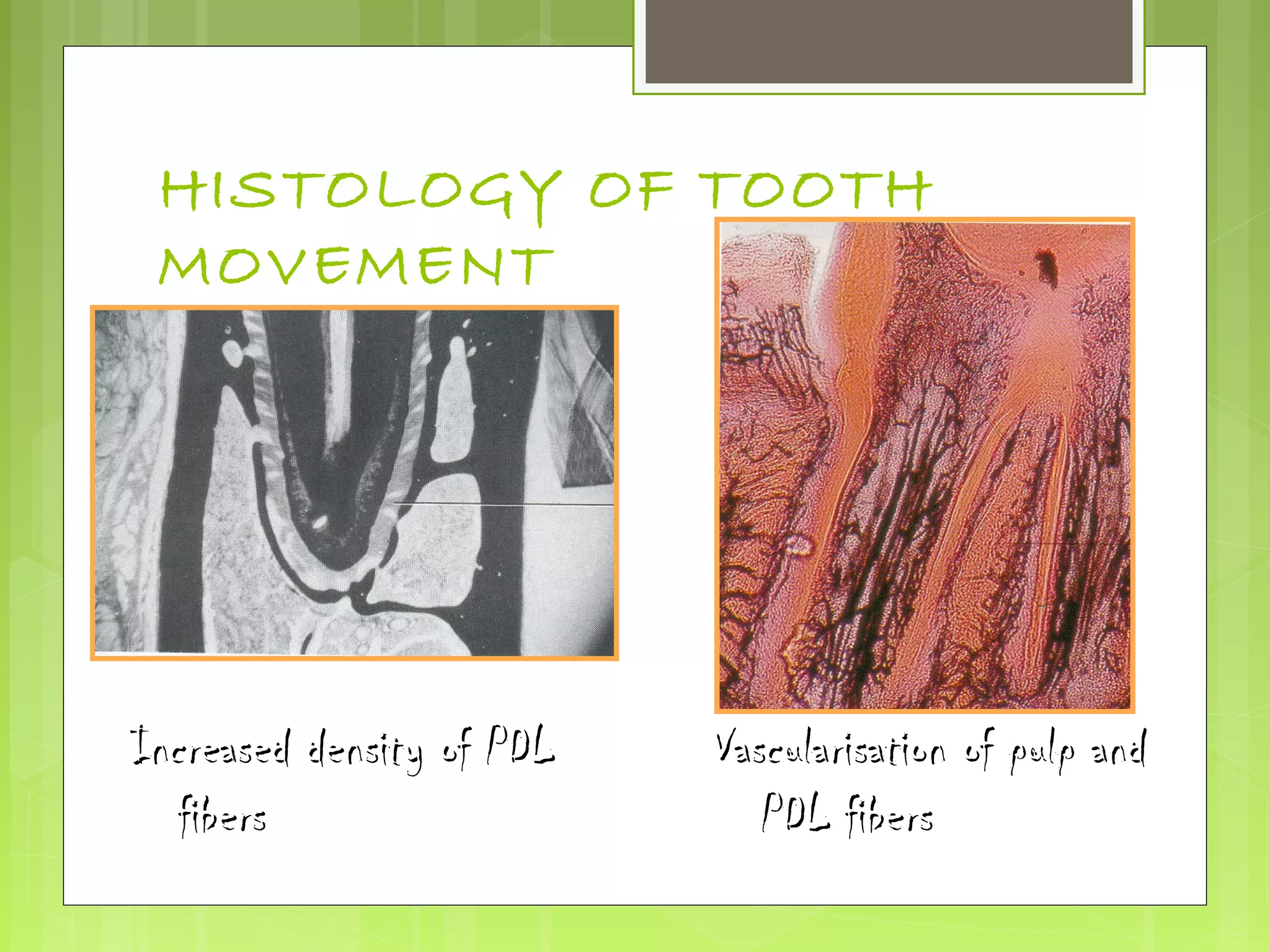
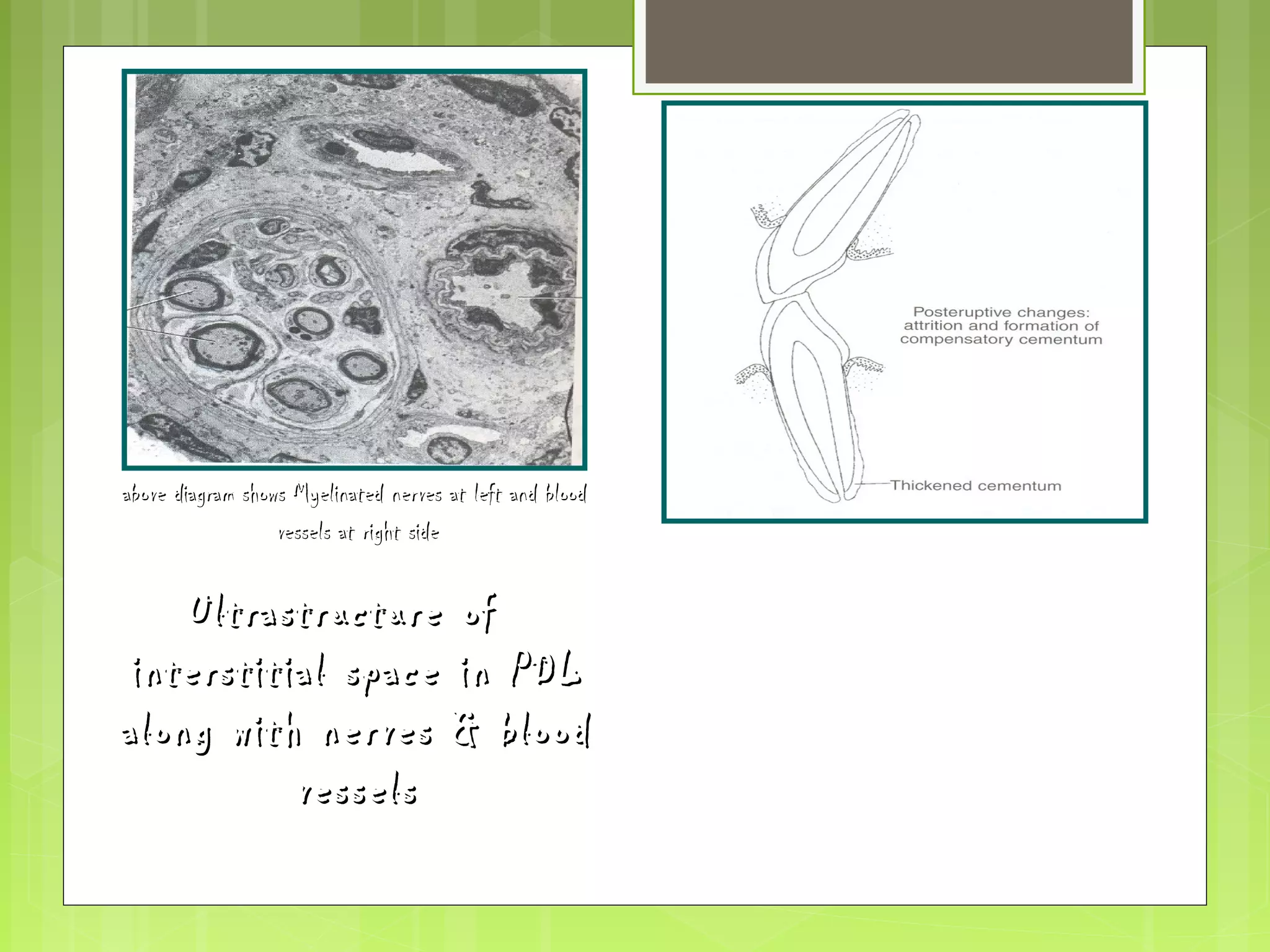
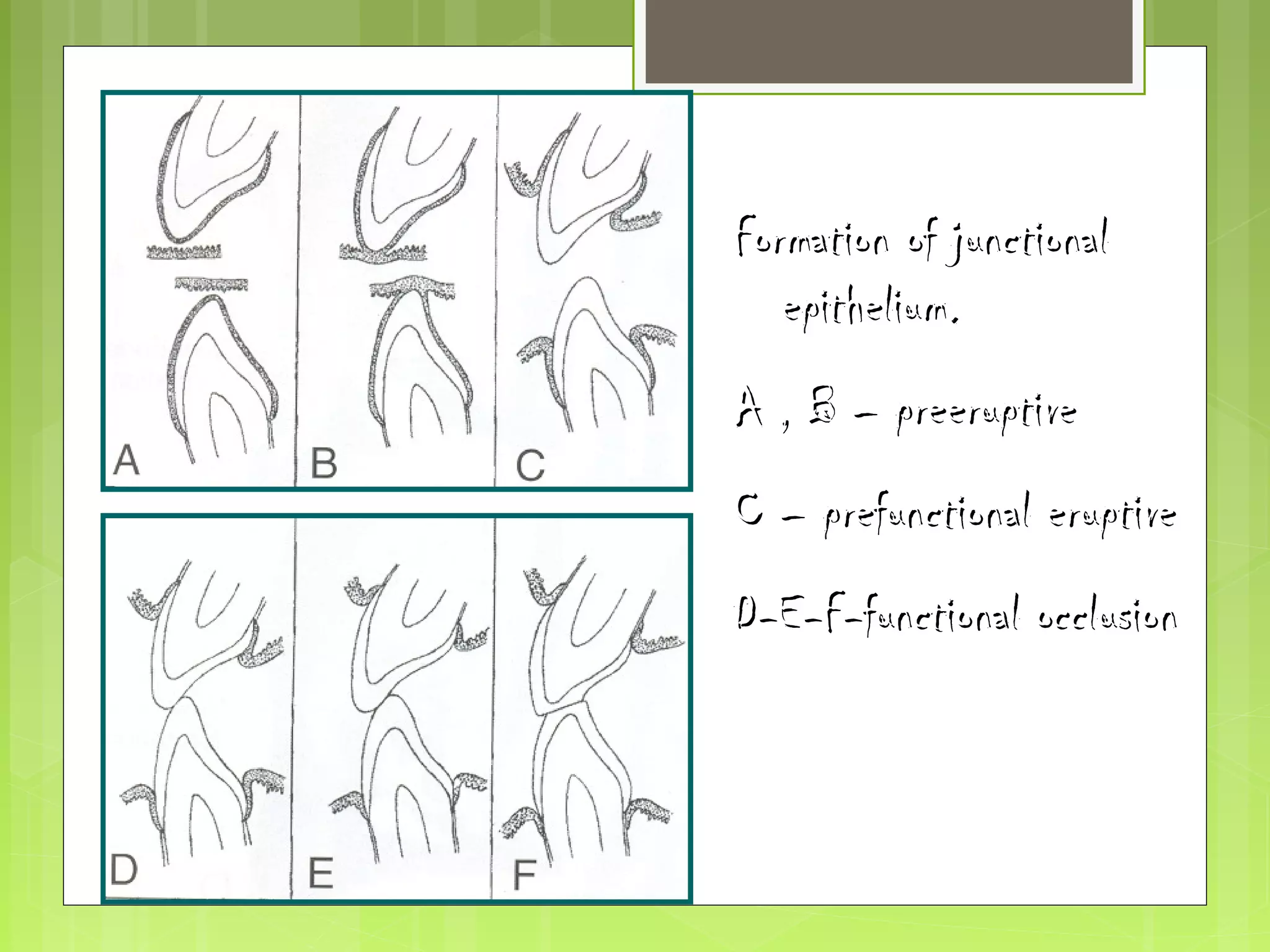
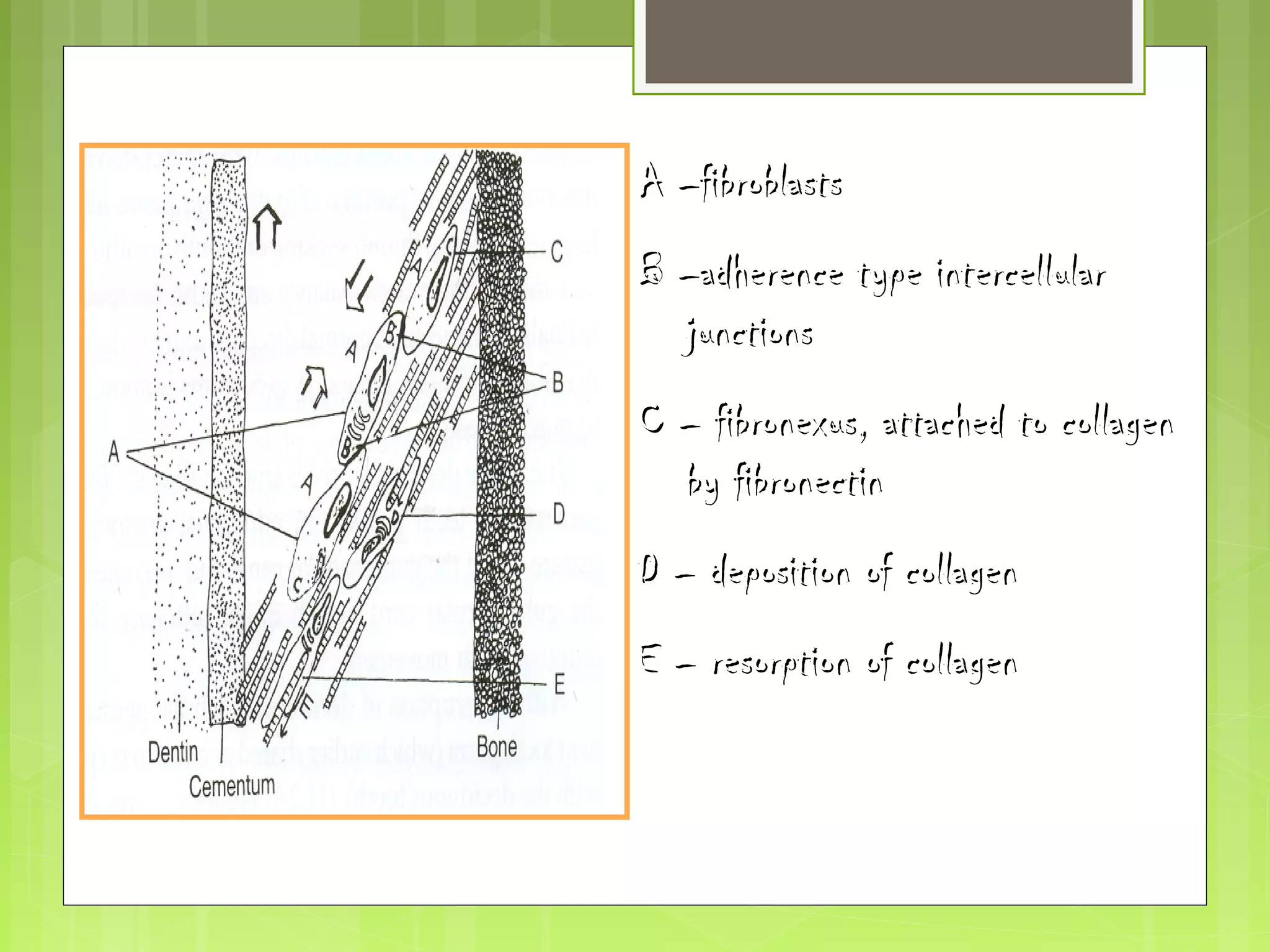




The document discusses tooth eruption and shedding. It defines tooth eruption and describes the various stages of eruption including pre-eruptive, eruptive, and posteruptive movements. It discusses the patterns, histology, and theories of tooth eruption. Key stages include pre-eruptive tooth movements within the jaw, eruption through the bone and oral mucosa, and posteruptive movements to maintain position. Theories discussed include bone remodeling, root growth, hydrostatic pressure, and periodontal ligament traction.