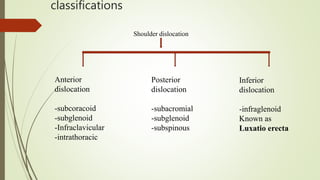
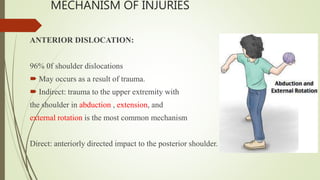
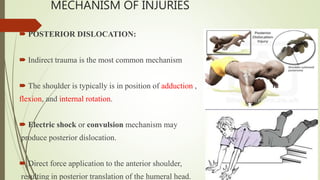
- Shoulder dislocations are commonly caused by trauma that places the shoulder in positions of extreme range of motion. Anterior dislocations are the most common type.
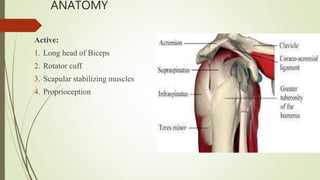
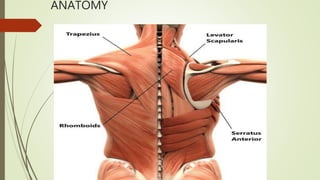
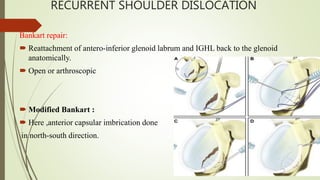
- The shoulder joint is inherently unstable due to its anatomy, relying on both passive structures like the labrum and ligaments as well as active stabilizers like muscles.
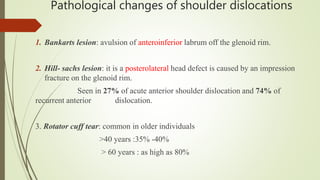
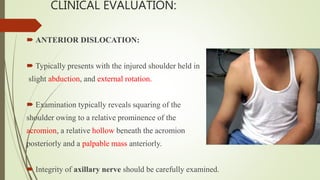
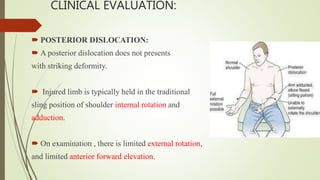
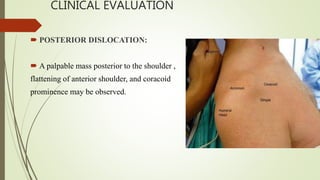
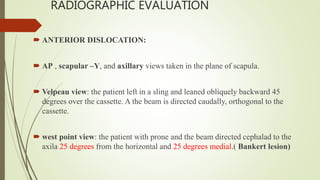
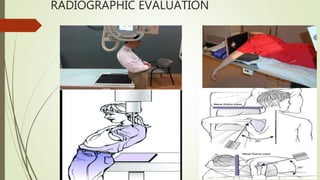
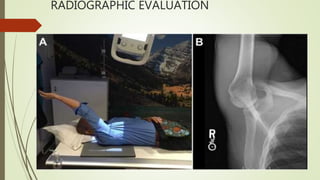
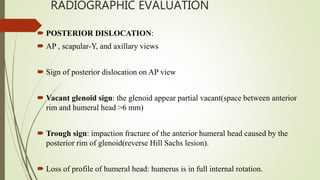
- Clinical evaluation and radiographs are used to diagnose the type of dislocation and assess for complications like fractures.
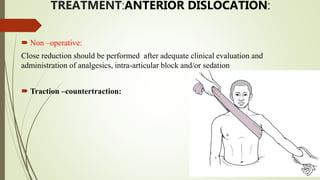
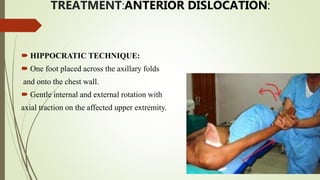
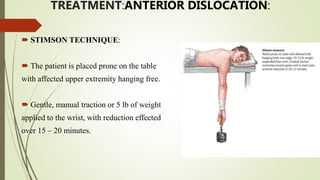
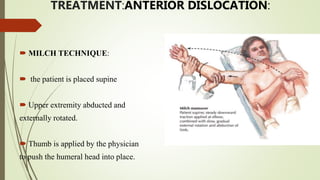
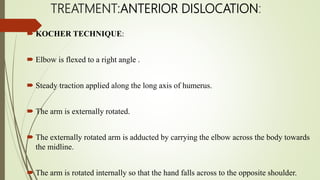
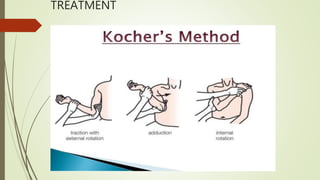
- Treatment involves closed reduction for most acute dislocations. Recurrent or complicated dislocations may require surgery and immobilization followed by physical therapy.