Prof. Dr. ÖzgürDeren
Hacettepe Üniversitesi Tıp Fakültesi
Kadın Hastalıkları ve Doğum ABD
Perinatoloji ve Maternal Fetal Tıp Ünitesi
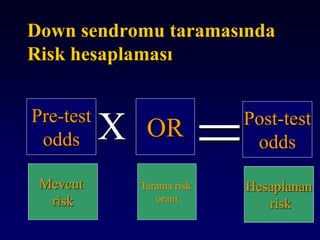
Gebelikte Tarama Testlerinin Temel
Dayanakları
2.
Konuşma planı I
•Sensitivite
• Spesifite
• PPD
• NPD
• LR
• Cut-off bulma
• ROC curve
3.
Konuşma planı II
•Neural tüp defekti taraması
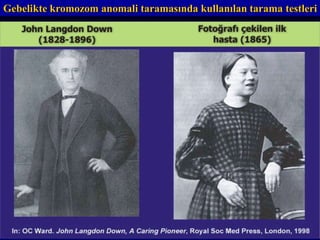
• Down sendromu taraması
• Gestasyonel diabet taraması
• Enfeksiyon taraması
• Antenatal kardiotokografi (NST)
Tarama testi tanımı
•Görünüşe göre iyi olan gruptan belli bir
hastalığın (veya durumun)
• bulunma olasılığının yüksek olduğu kişileri
ortaya koymağa yönelik yapılan
• organize girişimlerdir.
Başarılı bir taramaprogramı için
gerekli özellikler I
• Hastalığın erken tedavisi olmalı
• Taranan hastalığın doğal seyri bilinmeli
• Yarar maliyet etkin olmalı
8.
Başarılı bir taramaprogramı için
gerekli özellikler II
• Toplum için önemli olmalı
-Prevalans
• Geçerli ve güvenilir test olmalı
• Toplum tarafından benimsenmeli
• Tanıyı onaylaycak imkan olmalı
9.
Taramada hedef kitle
•Tüm populasyon
• Hedef populasyon
– Belli yaş grubu (mamografi)
– Belli klinik durum (gebelik)
Likelihood oranları (LR)
LR+ =
sensitivite
1-spesifisite
LR =
1-sensitivite
spesifisite
Testin performansını anlatmada kullanılır.
LR hastalık olanlarda bir testin sonucunun hastalık olmayanlara
göre kaç misli fazla (LR(+)) veya az (LR(-)) olduğunu gösterir
18.
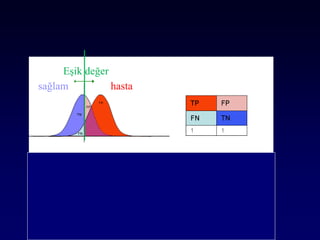
Taramada eşik değerlernasıl
bulunur ?
• 50 gr da: 140 mg/dl
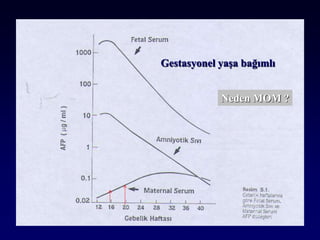
• AFP: 2.5 MoM
• Üçlü test: 1:270
19.
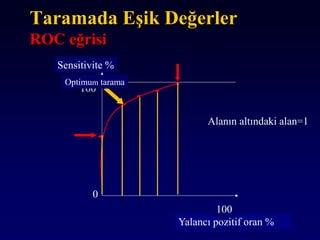
Taramada Eşik Değerler
ROCeğrisi
Sensitivite %
Yalancı pozitif oran %
0
100
100
Optimum tarama
Alanın altındaki alan=1
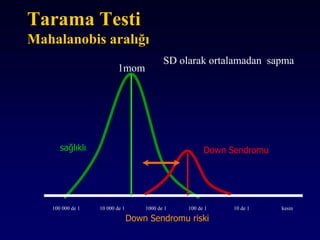
Tarama Testi
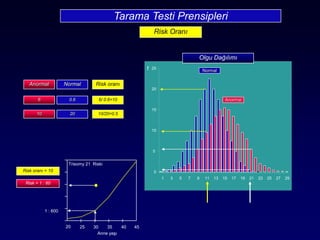
Mahalanobis aralığı
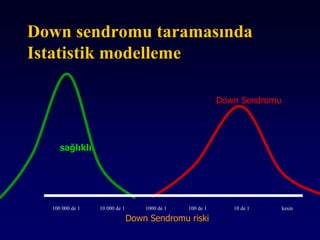
sağlıklıDown Sendromu
Down Sendromu riski
100 000 de 1 10 000 de 1 1000 de 1 100 de 1 10 de 1 kesin
SD olarak ortalamadan sapma
1mom
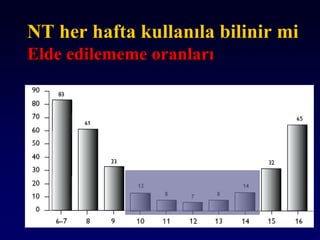
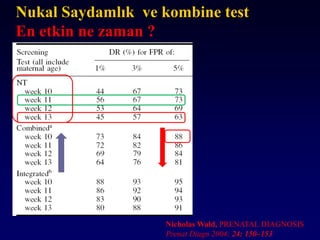
NT her haftakullanıla bilinir mi
Elde edilememe oranları
40.
Nicholas Wald, PRENATALDIAGNOSIS
Prenat Diagn 2004; 24: 150–153
Nukal Saydamlık ve kombine test
En etkin ne zaman ?
41.
7 8 910 11 12 13 14 15 16 17 18 19 20
Kombine test
İkili test
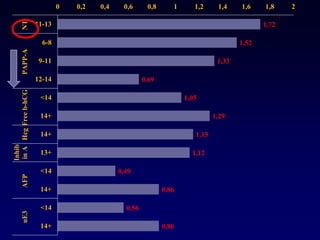
F-ᵦHcg
PAPP-A
Genetık Sono
NT
NB-DV-TY
2trim Bio
lu testHcg
AFP
uE
Inhibin
Hangi testler mevcut ?
42.
11 12 1314 15 16 17 18 19 20
İkili test
F-ᵦHcg
PAPP-A
NT
2trim Bio
lu testHcg
AFP
uE
Inhibin
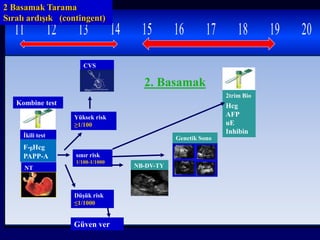
2 Basamak Tarama
Sıralı ardışık (contingent)
Kombine test
Yüksek risk
≥1/100
Düşük risk
≤1/1000
sınır risk
1/100-1/1000
CVS
Güven ver
NB-DV-TY
2. Basamak
Genetik Sono
43.
7 8 910 11 12 13 14 15 16 17 18 19 2
Her iki testi herkese
yapalım mı ?
Gestasyonel yaş
AFP+Hcg+uE+İnhibin
Triple
veya
Dörtlü test
NT
Serbest hcg
PAPP-A
Kombine test
Amnio
Yüksek risk
≥1/270
Güven ver
Düşük risk
ör≤1/270
Yüksek risk
≥1/300
CVS
Düşük risk
Yalancı pozitiflik %17
Sensitivite %98
44.
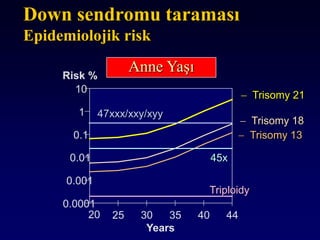
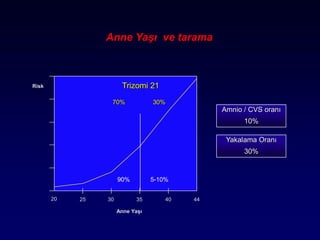
Anne Yaşı vetarama
Amnio / CVS oranı
10%
20 25 30 35 40 44
Anne Yaşı
Risk Trizomi 21
70% 30%
5-10%90%
Yakalama Oranı
30%
45.
Gebelikte Tarama testiolarak
kullanılan diğer testler
TORCH
NST
Kan biokimyası
Rubella
Hemogram
HbsAg
46.
Test nedir ?
•Klinisyen olarak yapılan herşey
–Hikaye alma
–Muayene
–Fundus ölçme