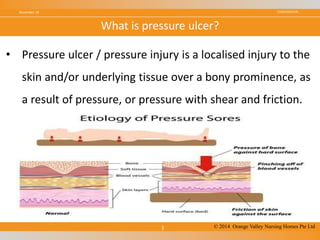
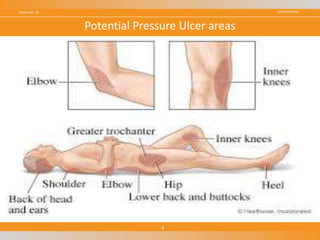
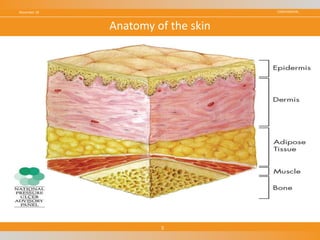
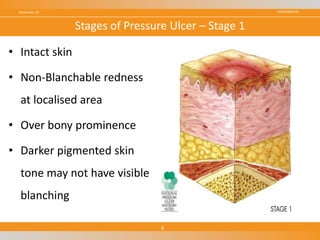
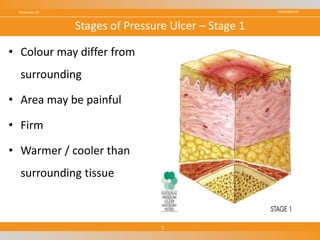
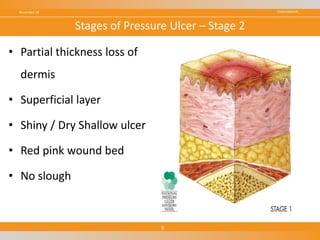
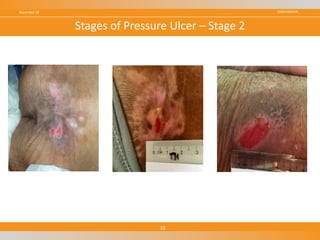
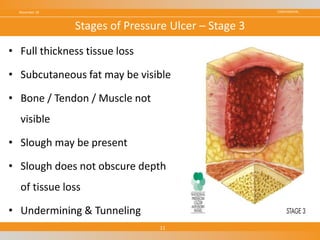
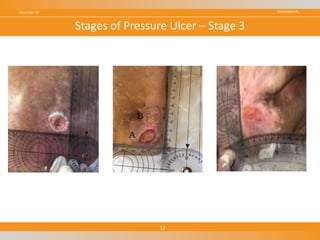
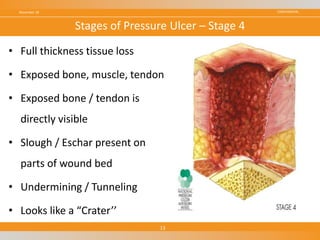
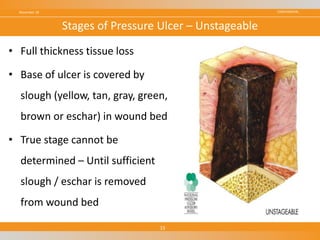
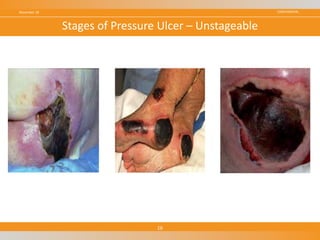
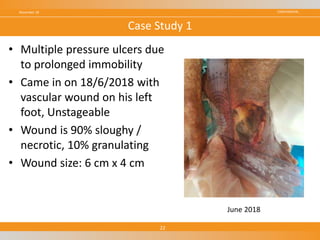
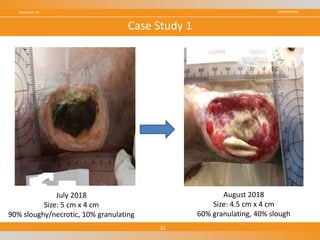
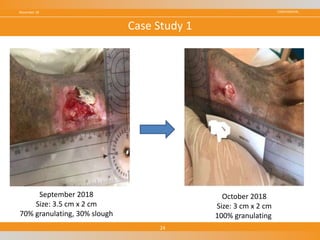
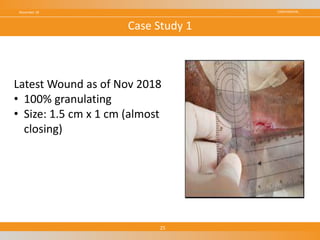
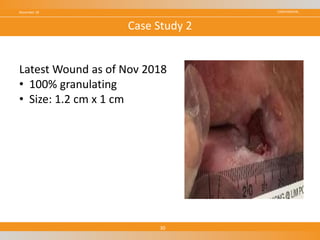
The document discusses pressure ulcers, including their definition, risk factors, stages, and case studies of management. It defines pressure ulcers as localized skin or tissue damage caused by prolonged pressure over bony areas. It outlines four stages of pressure ulcers based on depth of tissue damage. Two case studies are presented showing management of pressure ulcers through regular wound assessment, dressing changes, and multidisciplinary care including nutrition and physical therapy support. Prevention strategies emphasized include skin inspection, repositioning, and use of pressure-relieving surfaces.