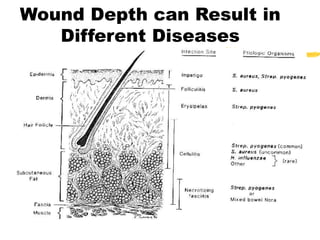
This document discusses the microbiology of chronic wounds. It begins by stating that all chronic wounds are contaminated by bacteria, though some bacteria may aid healing. It defines wound contamination, colonization, and infection. The microbial flora of wounds changes over time, initially containing normal skin flora and later more pathogens. Chronic wounds contain more anaerobes. Factors like bacterial dose, virulence, and host resistance determine if a wound becomes infected. Specimen collection by biopsy is ideal to diagnose infection.






















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













