WHAT ARE VITAMINS?
Essential organic compounds that are required in small amounts for
normal growth, maintenance of good health and for the proper utilization
of other nutrients.
Nutrients that our body does not make on its own. Thus we must obtain
them from the foods we eat, or via vitamin supplements.
3.
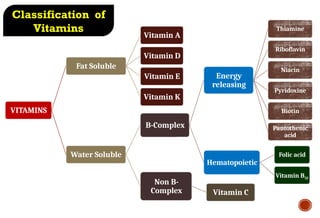
VITAMINS
Fat Soluble
Vitamin A
VitaminD
Vitamin E
Vitamin K
Water Soluble
B-Complex
Energy
releasing
Thiamine
Riboflavin
Niacin
Pyridoxine
Biotin
Pantothenic
acid
Hematopoietic
Folic acid
Vitamin B12
Non B-
Complex Vitamin C
Classification of
Vitamins
4.
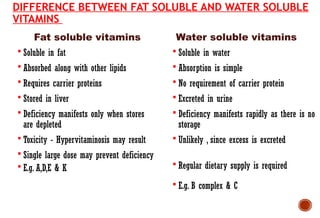
Fat soluble vitamins
DIFFERENCEBETWEEN FAT SOLUBLE AND WATER SOLUBLE
VITAMINS
Soluble in fat
Absorbed along with other lipids
Requires carrier proteins
Stored in liver
Deficiency manifests only when stores
are depleted
Toxicity - Hypervitaminosis may result
Single large dose may prevent deficiency
E.g. A,D,E & K
Soluble in water
Absorption is simple
No requirement of carrier protein
Excreted in urine
Deficiency manifests rapidly as there is no
storage
Unlikely , since excess is excreted
Regular dietary supply is required
E.g. B complex & C
Water soluble vitamins
5.
Hydrophobic
Isoprene derivatives
They cannotbe synthesized by the body
Supplied by the diet
Absorption along with fat
Transport: By lipoprotein & Specific binding protein
Surplus amount stored – liver & adipose tissue
Excess consumption leads to accumulation & toxic effects.
Lipid soluble vitamins - common features
Introduction
• Vitamin Ais an essential nutrient needed in small
amounts for the normal functioning of the visual
system, and maintenance of cell function for growth,
epithelial integrity, red blood cell production,
immunity and reproduction.
• Vitamin A deficiency (VAD) is a major nutritional
concern in poor societies, especially in lower income
countries like INDIA.
VITAMIN A
(PREFORMED ANDPROVITAMIN)
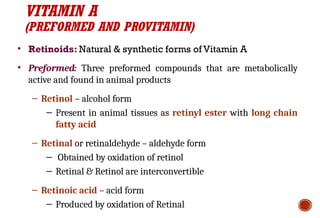
• Retinoids: Natural & synthetic forms of Vitamin A
• Preformed: Three preformed compounds that are metabolically
active and found in animal products
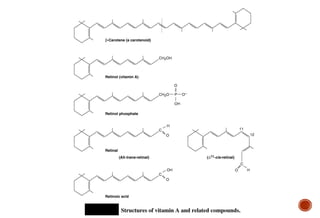
– Retinol – alcohol form
– Present in animal tissues as retinyl ester with long chain
fatty acid
– Retinal or retinaldehyde – aldehyde form
– Obtained by oxidation of retinol
– Retinal & Retinol are interconvertible
– Retinoic acid – acid form
– Produced by oxidation of Retinal
10.
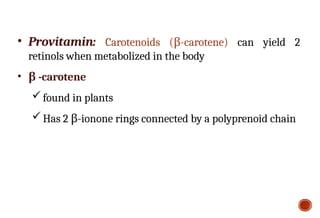
• Provitamin: Carotenoids(β-carotene) can yield 2
retinols when metabolized in the body
• β -carotene
found in plants
Has 2 β-ionone rings connected by a polyprenoid chain
13.
RECOMMENDED DAILY ALLOWANCE:
The recommended daily allowance of vitamin A is as follows:
(i) Infants 300-400 μg;
(ii) children 400-600 μg;
(iii) adolescents 750 μg;
(iv) pregnant women 800 μg.
1 μg retinol equivalent (RE) = 3.3 international units (IU) of vitamin A. Hence,
30 mg retinol = 100,000 IU vitamin A.
14.
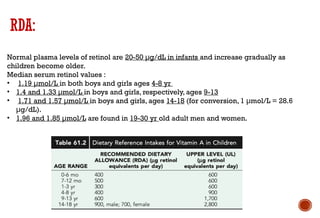
RDA:
Normal plasma levelsof retinol are 20-50 μg/dL in infants and increase gradually as
children become older.
Median serum retinol values :
• 1.19 μmol/L in both boys and girls ages 4-8 yr
• 1.4 and 1.33 μmol/L in boys and girls, respectively, ages 9-13
• 1.71 and 1.57 μmol/L in boys and girls, ages 14-18 (for conversion, 1 μmol/L = 28.6
μg/dL).
• 1.96 and 1.85 μmol/L are found in 19-30 yr old adult men and women.
15.
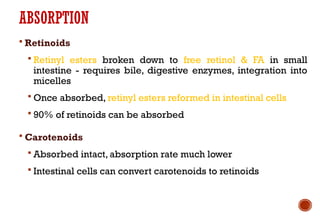
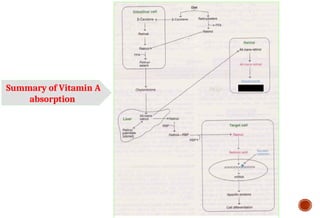
ABSORPTION
Retinoids
Retinylesters broken down to free retinol & FA in small
intestine - requires bile, digestive enzymes, integration into
micelles
Once absorbed, retinyl esters reformed in intestinal cells
90% of retinoids can be absorbed
Carotenoids
Absorbed intact, absorption rate much lower
Intestinal cells can convert carotenoids to retinoids
16.
Approximately 80% isabsorbed.
It is passed along with fat through the lymphatic
system into blood stream.
Absorption is poor in case of diarrhea, jaundice and
abdominal disorder.
Absorption increases if taken with fat.
Vitamin A which is not absorbed is excreted within 1
or 2 days in feces .
17.
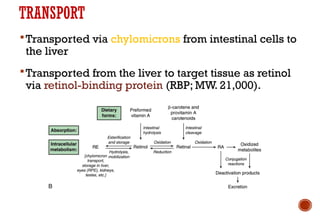
TRANSPORT
Transported via chylomicronsfrom intestinal cells to
the liver
Transported from the liver to target tissue as retinol
via retinol-binding protein (RBP; MW. 21,000).
STORAGE
The liver hasenormous capacity to store in the
form of retinol palmitate.
Under normal conditions a well-fed person has
sufficient Vitamin A reserves to meet his need for
6 to 9months or more.
21.
EXCRETION OF VITAMINA
Not readily excreted
Kidney disease and aging increase risk of toxicity
because excretion is impaired
22.
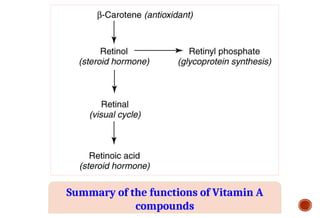
FUNCTIONS OF VITAMINA
Vision: Vitamin A is a component of the visual pigment
rhodopsin. Retinal is bound to the protein opsin.
Growth: Vitamin A deficiency causes loss of appetite. Slow bone
growth. Affects CNS.
Reproduction: Essential for spermatogenesis, oogenesis,
placental development, fetal & embryonic growth.
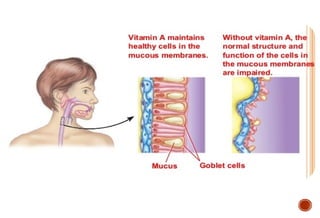
Maintenance of epithelial cells: Essential for normal
differentiation of epithelial tissues and mucus secretion
23.
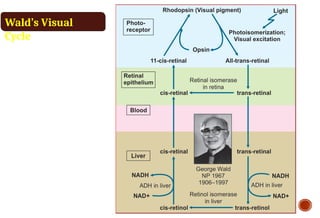
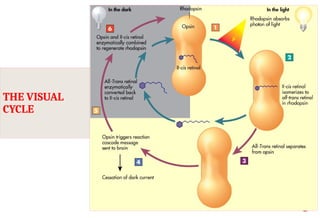
ROLE OF VITAMINA IN VISION
Visual Cycle (Wald’s Visual Cycle)
A process by which light impacting on the retina of
the eye is converted to an electrical signal
The optic nerve carries the electrical signal to the
brain (nerve impulse)
The brain processes the signal into an image
24.
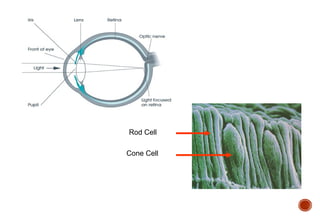
ROLE OF VITAMINA IN VISION
Retina is a light-sensitive layer of cells at the back of
the eye where an image is formed
Retina consists of: Rod and cone cells (photosensitive
cells)
Rod cells process black & white image
Cone cells process color image
ROLE OF VITAMINA IN VISION
Normal vision depends on the retina and on
adequate vitamin A
In the retina, vitamin A in the form of retinal binds to
a protein called opsin to make rhodopsin [11-cis –
retinal- opsin] in rod cells
Rhodopsin is a light-sensitive pigments
27.
ROLE OF VITAMINA IN VISION
The human retina contains 2 distinct photoreceptor systems: the rods, in
which rhodopsin senses light of low-intensity, and the cones, in which
iodopsins detect different colors; 11-cis-retinal is the prosthetic group on
both these visual proteins.
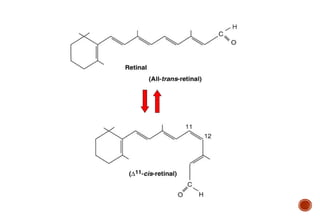
The mechanism of vitamin A action is similar for rods and cones, based on
photoisomerization of 11-cis to all-trans retinal (change shape when
exposed to light), which initiates signal transduction via the optic nerve to
the brain, resulting in visual sensation.
After isomerization (also known as photobleaching), a series of reactions
serves to regenerate the 11-cis retinal for resynthesis of rhodopsin and
iodopsin.
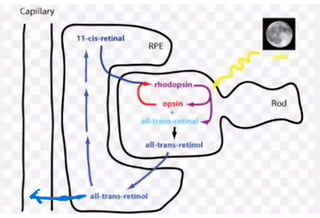
ROLE OF VITAMINA IN VISION
When stimulated by light, vitamin A isomerizes from
its bent ‘cis’ form to a straighter ‘trans’ form and
detaches from opsin
The opsin molecule changes shape, which sends a
signal to the brain via optic nerve and an image is
formed
Most retinal released in this process is quickly
converted to trans-retinol and then to cis-retinal, to
begin another cycle
32.
ROLE OF VITAMINA IN VISION
Dark Adaptation time
Bright light depletes rhodopsin (photobleaching)
Sudden shift from bright light to darkness causes
difficulty in seeing
Rhodopsin is synthesized in a few minutes and
vision is improved in the dark
33.
ROLE OF VITAMINA IN VISION
The time required to synthesize rhodopsin in the
dark is called dark adaptation time
It is increased in vitamin A deficiency
34.
FUNCTIONS OF VITAMINA:
GROWTH AND DIFFERENTIATION OF CELLS
• Retinoic acid is necessary for cellular differentiation
• Important for embryo development, gene expression
• Retinoic acid influences production, structure, and function
of epithelial cells that line the outside (skin) and external
passages (mucus forming cells) within the body.
35.
EPITHELIAL CELL ‘INTEGRITY’
Manyepithelial cell require Vitamin A for proper
differentiation and maintenance
Lack of Vitamin A leads to dysfunction of epithelia
The skin becomes keratinized and scaly, and mucus secretion is suppressed
37.
FUNCTIONS OF VITAMINA: IMMUNITY
Deficiency leads to decreased resistance to infections
Supplementation may decrease severity of infections in
deficient person
38.
Role in Preventionof cardiovascular disease
Antioxidant capabilities
Role in Cancer prevention
Antioxidant capabilities
Lung, oral, and prostate cancers
Studies indicate that vitamin A-containing foods are
more protective than supplements
39.
VITAMIN A DEFICIENCYAND DISEASES
Nyctalopia (night blindness)
Xerophthalmia
Bitot’s spots
Keratomalacia
Complete blindness (in severe deficiency)
40.
WHO CLASSIFICATION OFXEROPTHALMIA AS
FOLLOWING:
a) X1A – conjunctiva Xerosis (ocular epithelium becomes dry.)
b) X1B- Bitots spots (foam like hyper keratinized silvery lesions)
c) X2- corneal xerosis
d) X3A – corneal ulceration
e) X3B – Keratomalacia (hyper keratinization of cornea with corneal
opacity, which can progress to ulceration and infection)
f) XN- night blindness
g) XS – corneal scarring
h) XF- fundoscopic changes
41.
NIGHT BLINDNESS
Visualacuity is diminished in dim
light
Occurs as a result of inadequate
pigment in the retina.
The dark adaptation time is
increased
Found in pregnant women in some
instances, especially during the last
trimester of pregnancy when the
vitamin A needs are increased.
42.
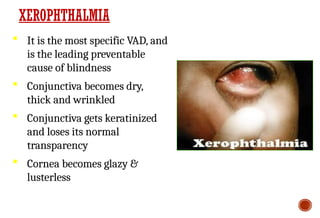
It isthe most specific VAD, and
is the leading preventable
cause of blindness
Conjunctiva becomes dry,
thick and wrinkled
Conjunctiva gets keratinized
and loses its normal
transparency
Cornea becomes glazy &
lusterless
XEROPHTHALMIA
43.
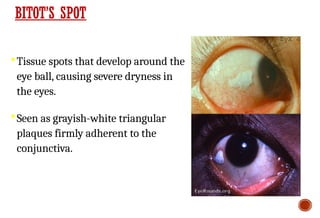
BITOT’S SPOT
Tissue spotsthat develop around the
eye ball, causing severe dryness in
the eyes.
Seen as grayish-white triangular
plaques firmly adherent to the
conjunctiva.
44.
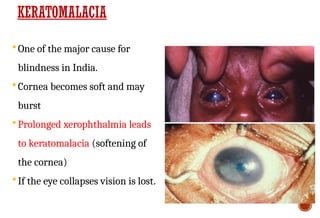
KERATOMALACIA
One ofthe major cause for
blindness in India.
Cornea becomes soft and may
burst
Prolonged xerophthalmia leads
to keratomalacia (softening of
the cornea)
If the eye collapses vision is lost.
45.
Follicular hyperkeratosis
Anorexia
Growth retardation
Increased respiratory & intestinal infection
Defective tooth enamel
Reproductive failure.
OTHER SYMPTOMS OF VAD
46.
TREATMENT:
More often,higher doses of 30-60 mg of retinol (100,000-200,000
IU/child) are given once or twice, under careful monitoring to avoid
toxicity associated with excess vitamin A.
Xerophthalmia is treated by giving 1,500 μg/kg body weight orally
for 5 days, followed by intramuscular injection of 7,500 μg of vitamin
A in oil, until recovery.
< 6 months: 50,000 IU
6 months – 12 months: 1,00,000 IU
>12 months: 2,00,000 IU
48.
PREVENTION:
Vitamin Adeficiency is a public health problem in India.
The Ministry of Health and Family Welfare initiated the 'National
Prophylaxis Program against Nutritional Blindness' in 1970.
According to this scheme, children between 9 months and 3 years
were given oral doses of vitamin A every six months. It was later
expanded to cover children of ages 6-59 months.
Under this program, a dose of vitamin A 100,000 IU is given with
measles vaccine at 9 months and 2,00,000 IU with DPT booster at 15-
18 months and then 6monthly till 5 years of age.
Children with measles or severe malnutrition should receive vitamin
A at 100000 IU if < 1 year old and 200000 IU if older. As it decreases
mortality.
1) Eating ofpolar bear liver
2) Excess supplementation of
Vitamin A
When?
TOXICITY
One ounce of polar bear liver contains
enough vitamin A (retinol) to kill a
person!
HYPERVITAMINOSIS A:
Chronicdaily intakes of 15,000 μg (adults) and 6,000 μg (children) can
be toxic. Because there is no antidote for hypervitaminosis A, and
vitamin A is readily stored in liver and other tissues.
Extreme hypervitaminosis A is fatal.
Signs of subacute or chronic toxicity can include:
headache, vomiting (early signs), anorexia, dry itchy desquamating
skin, and seborrheic cutaneous lesions.
With chronic hypervitaminosis A,
fissuring at the corners of the mouth, alopecia and coarsening of the
hair, bone abnormalities and swelling, enlargement of the liver and
spleen, diplopia, increased intracranial pressure, irritability, dryness
of the mucous membranes, and desquamation of the palms and the
soles of the feet.
53.
Less commonsymptoms include diplopia, papilledema,
cranial nerve palsies, and other symptoms suggesting
pseudotumor cerebri.
Teratogenicity has been associated with therapeutic doses
(0.5-1.5 mg/ kg) of oral 13-cis-retinoic acid, generally taken
for the treatment of acne or cancer, during the 1st trimester
of pregnancy.
A high incidence (>20%) of spontaneous abortions and
birth defects, including characteristic craniofacial
abnormalities.
Carotenoids can cause yellowing of the skin
(carotenodermia).
![ROLE OF VITAMIN A IN VISION
Normal vision depends on the retina and on
adequate vitamin A
In the retina, vitamin A in the form of retinal binds to
a protein called opsin to make rhodopsin [11-cis –
retinal- opsin] in rod cells
Rhodopsin is a light-sensitive pigments](https://image.slidesharecdn.com/vitafinal-260120175651-b972f740/85/VIT-A-FINAL-pptxbBsbbsbsbsbsbsbbsbsbbsbsbsbbs-26-320.jpg)
























![M. Fat soluble vitamins 1[1].pptx BS BIOCHEMISTRY](https://cdn.slidesharecdn.com/ss_thumbnails/m-250422132531-17f74db5-thumbnail.jpg?width=640&height=640&fit=bounds)
































