
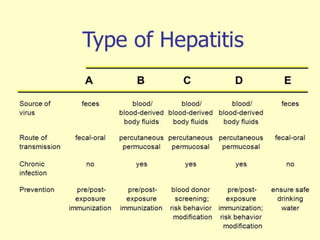


The document discusses viral hepatitis, detailing its types (A, B, C, D, and E), their transmission modes, clinical features, and diagnostic methods. Hepatitis A is primarily spread through contaminated food and water, while Hepatitis B and C are transmitted via blood and bodily fluids, with distinct risks for chronic infection and different treatment options. Prevention strategies include vaccination, immune globulin for post-exposure, and safe practices to mitigate risk factors, particularly for travelers to endemic regions.





























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)





