Hepatitis is inflammation of the liver caused by viral infections, drugs, toxins, autoimmune disease, or metabolic disorders. It may be acute or chronic.
Objectives
• Mention theetiologic agents of viral hepatitis.
• Discuss viral hepatitis (A,B,C,D,E) in terms of
pathogenesis, clinical manifestations and laboratory
diagnosis.
• List the complications of viral hepatitis.
• Define chronic hepatitis.
• List the etiologies, clinical features and lab findings of
chronic hepatitis.
• Define, mention the clinical presentation and lab
investigation of autoimmune hepatitis.
3.
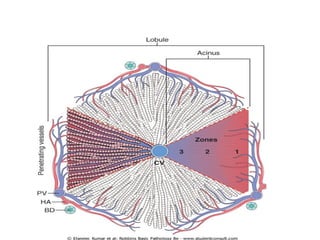
NORMAL MICROANATOMY OFTHE LIVER
• The functional unit of the liver is represented
by either:-
A. The hepatic lobule.
B. The hepatic acinus .
5.
• Chronic inflammatorydisorders of the liver
dominate the clinical practice of hepatology.
• Virtually any insult to the liver can kill hepatocytes
and recruit inflammatory cells.
Liver infections:
1. Viral hepatitis.
2. Autoimmune hepatitis.
3. Others, miliary tuberculosis, malaria,
salmonelloses, candidiasis, and amebiasis.
6.
Systemic viral infectionsinclude:-
1) Infectious mononucleosis (Epstein-Barr virus).
2) Cytomegalovirus or herpesvirus infections in the newborn
or immunosuppressed.
3) Yellow fever,cause hepatitis in tropical countries.
4) Infrequently, rubella, adenovirus, or enterovirus infections.
However, unless otherwise specified, the term viral
hepatitis is reserved for primary infection of the liver
caused by a small group of viruses having a particular
affinity for the liver (hepatotropes).
7.
Viral Hepatitis
• Theetiologic agents of viral hepatitis:-
1. Hepatitis A virus (HAV).
2. Hepatitis B virus (HBV).
3. Hepatitis C virus (HCV).
4. Hepatitis D virus (HDV).
5. Hepatitis E virus (HEV).
8.
Hepatitis A (infectioushepatitis)
• Is a benign, self-limited disease with an
incubation period of 15 to 50 days (aveg.28days).
• HAV has the largest potential among the hepatitis
viruses to cause epidemics in countries with poor
hygiene and sanitation, so that most natives of
such countries have detectable antibodies to HAV
by the age of 10 years.
9.
• Classification:-
HAVRNA picornavirus.
• Pathogenesis:-
It reaches the liver from the intestinal tract after ingestion,
replicates in hepatocytes, and is shed in the bile and feces.
The virus itself does not seem to be toxic to hepatocytes,
and hence the liver injury seems to result from T cell-
mediated damage of infected hepatocytes.
Immunoglobulin M (IgM) antibodies against HAV that
appear in blood at the onset of symptoms.
10.
• Investigations:-
Detectionof anti-HAV IgM antibody is the best
diagnostic marker for the disease.
• Prevention and management:-
1) Hygienic measures focused on the disposal of human
wastes and personal hygiene.
2) Passive immunization with immune serum globulin for
individuals exposed to the virus or those traveling to
high-exposure areas.
3) Immunization using a virus-inactivated vaccine.
11.
Hepatitis B Virus(HBV)
• Classification:-
HBV DNA virus is a member of the Hepadnaviridae
The incubation period is 4 to 26 weeks.
• Transmission:-
It presents in all physiologic and pathologic body
fluids(with the exception of stool) such as semen, saliva,
sweat, tears, breast milk, and pathologic effusions.
• HBV is a hardy virus and can withstand extremes of
temperature and humidity.
12.
• In endemicregions:-
vertical transmission from mother to child during
birth constitutes the main mode of transmission.
• In areas of low prevalence:-
Horizontal transmission via
Transfusion, blood products.
Dialysis.
Needle-stick accidents among health care workers.
Intravenous drug abuse.
Sexual transmission (homosexual or heterosexual) .
In one-third of patients the source of infection is unknown.
13.
Pathogenesis:-
• The mechanismsof innate immunity protect the
host during the initial phases of the infection,
and a strong response by virus-specific CD4+ and
CD8+ interferon γ-producing cells are associated
with the resolution of acute infection.
• HBV does not cause direct hepatocyte injury but
it believed to result from damage to the virus-
infected cells by CD8+ cytotoxic T cells.
14.
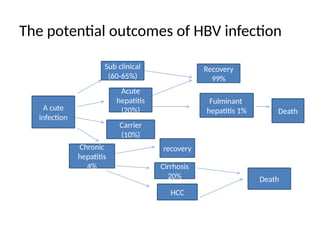
The potential outcomesof HBV infection
A cute
infection
Sub clinical
(60-65%)
Acute
hepatitis
(20%)
Carrier
(10%)
Chronic
hepatitis
4%
recovery
Cirrhosis
20%
HCC
Death
Recovery
99%
Fulminant
hepatitis 1% Death
15.
• Prevention:-
1. Vaccination.
2.Screening of donor blood, organs, and
tissues.
The vaccine is prepared from purified HbsAg
produced in yeast.
16.
Hepatitis C Virus(HCV)
• Is a major cause of chronic liver disease.
• The worldwide carrier rate is estimated at 175 million persons.
• the most common risk factors for HCV infection are:
Intravenous drug abuse (54%)
Multiple sex partners (36%)
Having had surgery within the last 6 month (16%)
Needle stick injury (10%)
Multiple contacts with an HCV-infected person (10%)
Employment in medical or dental fields (1.5%)
Unknown (32%)
17.
The incubation periodfor hepatitis C ranges from
2 to 26 weeks, with a mean of 6 to 12 weeks.
• Persistent infection and chronic hepatitis are the
hallmarks of HCV infection, despite the generally
asymptomatic nature of the acute illness.
• HCV RNA testing must be performed to assess
viral replication and to confirm the diagnosis of
HCV infection.
18.
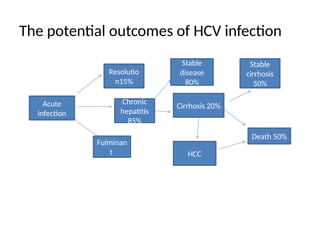
The potential outcomesof HCV infection
Acute
infection
Resolutio
n15%
Chronic
hepatitis
85%
Fulminan
t
Stable
disease
80%
Cirrhosis 20%
HCC
Stable
cirrhosis
50%
Death 50%
19.
Hepatitis D Virus(HDV)
• Also called hepatitis delta virus.
Delta hepatitis arises in two settings:
• (1) acute coinfection after exposure to serum
containing both HDV and HBV.
• (2) superinfection of a chronic carrier of HBV
with a new inoculum of HDV.
20.
IgM anti-HDV antibodyis the most reliable
indicator of recent HDV exposure.
• Nevertheless, acute coinfection by HDV and
HBV is best indicated by detection of IgM
against both HDV Ag and HBcAg (denoting
new infection with HBV).
21.
Hepatitis E Virus(HEV)
Is an enterically transmitted, waterborne infection
occurring primarily beyond the years of infancy.
HEV is endemic in Asia, sub-Saharan Africa, and Mexico.
A characteristic feature of the infection is the high
mortality rate among pregnant women, approaching
20%.
The average incubation period after exposure is 6 weeks
(range, 2-8 weeks).
Virus can be detected in stools, and anti-HEV IgG and
IgM antibodies are detectable in serum.
22.
Clinical Features andOutcomes of Viral
Hepatitis
• A number of clinical syndromes may develop after
exposure to hepatitis viruses:
1) Asymptomatic acute infection: serologic evidence only.
2) Acute hepatitis: anicteric or icteric.
3) Chronic hepatitis: with or without progression to
cirrhosis.
4) Chronic carrier state: asymptomatic without apparent
disease.
5) Fulminant hepatitis: submassive to massive hepatic
necrosis with acute liver failure.
23.
S &S
Nonspecificsymptoms like higher fever, shaking
chills, and headache, sometimes accompanied
by right upper quadrant pain .
Jaundice, predominantly conjugated
hyperbilirubinemia (dark-colored urine).
The stools may become light colored due to
cholestasis and pruritus.
And on physical examination there is mildly
enlarged, tender liver.
24.
Acute viral hepatitis
•The characteristic features of acute viral
hepatitis are:
• fever, anorexia, nausea, jaundice and
hepatomegaly associated with markedly
raised transaminases.
25.
Acute viral hepatitis
•Three clinical phases are recognised
1/ Prodromal phase.
There is malaise usually associated with fever, vomiting,
and abdominal pain.
Often the urine is dark, due to bilirubinuria, even
though jaundice is not as yet clinically evident and
the hyperbilirubinaemia is relatively mild. At this
stage the serum transaminase activities are very high.
26.
2/ Icteric phase.Clinical jaundice and marked
• hyperbilirubinaemia occur after 5 to 10 days
and may last up to 2 to 3 weeks. As the
jaundice begins to abate, the serum
transaminases also drop.
3/ Convalescent phase. As the jaundice
disappears so do the abdominal pain and
tenderness.
27.
Chronic Hepatitis
• Isdefined as symptomatic, biochemical, or
serologic evidence of continuing or relapsing
hepatic disease for more than 6 months, with
histologically documented inflammation and
necrosis.
28.
Chronic Hepatitis
• Besidehepatitis viruses(particularly HCV),
there are many other causes of chronic
hepatitis include:-
1. Wilson disease.
2. α1-antitrypsin deficiency.
3. Chronic alcoholism, drugs (isoniazid, α-
methyldopa, methotrexate).
4. Autoimmunity.
29.
The clinical featuresof chronic hepatitis:-
1. Fatigue .
2. Malaise.
3. Loss of appetite.
4. Mild jaundice.
Physical findings:-
1. A spider angiomas.
2. Palmar erythema.
3. mild hepatomegaly, and hepatic tenderness.
30.
Chronic Hepatitis
Laboratoryfindings:-
1. Prolongation of the prothrombin time.
2. Hypergammaglobulinemia.
3. Hyperbilirubinemia.
4. Mild elevations in alkaline phosphatase
levels.
31.
Autoimmune hepatitis
• Isa syndrome of chronic hepatitis in persons
with a heterogeneous set of immunologic
abnormalities. The histologic features are
indistinguishable from chronic viral hepatitis.
This disease may run an indolent or severe
course and typically responds dramatically to
immunosuppressive therapy.
32.
Autoimmune Hepatitis
• Featuresinclude:
1) Female predominance (70%).
2) Absence of serologic markers of a viral infection.
3) Elevated serum IgG (>2.5 g/dL).
4) High titers of autoantibodies in 80% of cases.
5) The presence of other forms of autoimmune
diseases including rheumatoid arthritis,
thyroiditis, and ulcerative colitis.
33.
Pathogenesis and MainClinical
Features:-
Autoimmune hepatitis can be divided into
three subtypes on the basis of the
autoantibodies:-
1. Circulating antinuclear antibodies.
2. Anti-smooth muscle antibodies, liver kidney
microsomal antibody.
3. Anti-soluble liver/pancreas antigen.
The main effectors of cell damage in
autoimmune hepatitis are believed to be
CD4+ helper cells.
34.
Autoimmune hepatitismay present with mild to severe
chronic hepatitis.
Investigations:-
Immunofluorescence or enzyme-linked immunosorbent
assays.
Response to immunosuppressive therapy is usually
dramatic, although a full remission of disease is unusual.
The overall risk of cirrhosis, the main cause of death, is
5%.
Editor's Notes
#7 HCV= has the most chronicity(chronic hepatitis can develop to cirrhosis and hepatocellular carcinoma)
#12 If infection is acquired in early infancy the chance to develop chronic hepatitis is high (more than 70%)
endemic =mean 10%of the population have the disease
endemic areas are southeast Asia
1/3 unknown دي نقطة مهمة
















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
